
Remember me

A total of 308 patients were involved in this study. All of the sampled patients responded to the interview for sociodemographic characteristics. The majority of patients, 85.4% (263), were classified as ASA classless or equal to II. Of all the study subjects, 47.4% were males (Table 1). The average mean age of the participants was 42.9 ± 16.6 years (with a minimum of 18 years and a max of 70 years), and 29% of patients were greater or equal to 55 years old (Table 1). Among the sampled patients, 87.1% (268) of them had preoperative Hgb ≥ 10 mg/dl. The patients were interviewed for the preoperative status of comorbidities, and Tables 1 and 2 highlight that three-fourths of the patients had no known comorbidity, and 13% (38), 5.2% (16), and 4.5% (14) of the clients had respiratory, cardiovascular, renal, and/or endocrine system, respectively.
Table 1 Baseline distribution of sociodemographic and clinical characteristics of the patients who underwent elective surgery under GATE at JMC, Jimma, Ethiopia, 2024Table 2 Descriptive data on the distribution of sociodemographic and clinical characteristics with extubation time status of the patients who undergone elective surgery under GATE at JMC (N = 308)Anesthesia and surgical-related data of the patients who underwent elective surgery under GATE at JMC, Jimma, Ethiopia, 2024Table 3 shows that 43%, 28%, and 29% of patients were done with a BSc anesthetist, MSc holder anesthetist, and anesthesiologist residents, respectively. Of all the patients, 54.2% (167), 18.2% (56), and 27.6% (85) received ketamine, ketofol, and propofol as induction agents, respectively. Among all, 81.5% (251) of the patients took opioids, and similarly, 17.5% (54) of the patients took benzodiazepine. More than half (57.8%) of the patients were maintained with halothane, and more than three-fourths (76.6%) of the patients) took both suxamethonium and vecuronium, whereas only 6.5% (20) of the patients took suxamethonium alone. The average mean of ETCO2 at the EOS was 37.4 ± 2.9 mmHg among total patients, and similarly, the average mean of body temperature at EOS was 35.9 ± 0.690 °C. During the study period, the most common type of surgery done was general surgery (general surgery out of the abdomen, 12.3% (38), and thorax-abdominal surgery, 24.4%) (75). Most of the procedures were done in the supine position (73.1%, followed by the prone (10.4%), and steeper Trendelenburg (6.5%), as shown in Table 3. Among the study subjects, 39.3% (121) of patients had < 500 ml estimated intraop blood loss, whereas 45.8% (141) and 14.9% (46) of the patients had 500–1000 ml and > 1000 ml of intraoperative estimated blood loss respectively (Table 3).
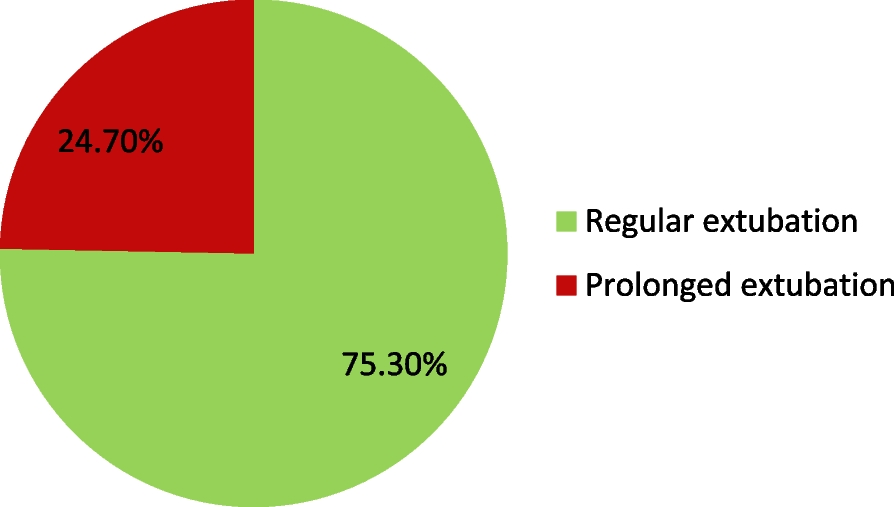
Table 3 Frequency distribution of anesthesia and surgery-related factors with extubation time status of the patients who undergone elective surgery under GATE at JMC (N = 308)Incidence of prolonged extubation time among the patients who underwent elective surgery under GATE at JMC, Jimma, Ethiopia, 2024The cumulative incidence of prolonged extubation time was 24.7%, 95% CI [20.0–29.9] (Fig. 1) and more common among the patients greater or equal to 55 years old (47.1% vs. 16%, p < 0.001) (Fig. 2). It was more frequent in respiratory comorbidities like COPD, asthma, lung cancer, and OSA compared to those with no known comorbidity (39.5% vs. 20.6%, p = 0.032). The patient with cardiovascular system comorbidity also had a higher incidence of PET than the patient with no known comorbidity (37.5% vs. 20.6%).
Fig. 1
Incidence of prolonged extubation time among adult patients who undergone elective surgery under GATE at JMC, 2024
Fig. 2
Extubation time status based on the age of patients among adult patients who undergone elective surgery under GATE at JMC, 2024. *ET, extubation time
There was a significant statistical association between anesthesia providers’ experience and the incidence of prolonged extubation time (p < 0.001) (Fig. 3). It was more frequent among patients who took BZD (50.9% vs. 19.3%, p < 0.001). The patients maintained with halothane had a higher cumulative incidence of PET compared to those who maintained with isoflurane (34.3% vs. 11.5%, p < 0.001). The incidence of PET was higher, 40% among patients who took low doses (0.01–0.03 mg/kg) of neostigmine and 23.5% among patients who took normal doses (0.031–0.07 mg/kg) of neostigmine(p = 0.032). The incidence of PET was more frequent among longer procedures (47.8% vs. 22.8%, p = 0.007). Both neurosurgery (45.5%, p < 0.001) and thoracoabdominal surgery patients showed a considerable incidence of PET (45.3%) (Table 3). The incidence of PET was higher among patients who were extubated afternoon (01:00 pm–7:00 pm) than those extubated morning (8:00 pm–1:00 pm) (37.1% vs. 16.3%) (Fig. 4).
Fig. 3
Extubation time status based on the anesthesia providers among adult patients who undergone elective surgery under GATE at JMC, 2024. *RET, regular extubation time; PET, prolonged extubation time
Fig. 4
Extubation time status based on the hour at which patients were extubated among adult patients who undergone elective surgery under GATE at JMC, 2024
Factors associated with PET among elective adult patients operated under GATE at JMC, Oromia, Ethiopia, 2024In bivariate analysis age of patients, sex, preexisting comorbidities, ASAPS, BMI, anesthesia providers, use of BDZ, use of opioids, type of maintenance agent used, position during operation, type/site of surgery, type of muscle relaxant used, amount of IV fluid given, intraoperative estimated blood loss, body temperature at the EOS, hour at which patient was extubated, and duration of operation were candidates for multivariate regression (Table 4). The correlation between those independent variables was checked for multicollinearity effect, by using variance inflation factor (VIF) and tolerance test for those p-values < 0.25. Duration of anesthesia and surgical procedure duration have statistically significant multicollinearity, and duration of anesthesia goes with the duration of procedure. Moreover, in this data, the duration of anesthesia was dependent on the duration of the procedure; so, the duration of surgery was included in the multivariate logistic regression. The results of multivariate logistic regression showed that the age of the patients, BMI, ASAPS, anesthesia providers, inhalational agents used, use of BDZ, position during surgery, an hour at which the patient was extubated, and duration of surgery had a statistically significant association with PET at a p-value ≤ 0.05 (Table 4). Eight of the factors that were statistically significant in bivariate regression, including gender, preoperative comorbidity, intraoperative estimated blood loss, opioid use, amount of IV fluid given, type/site of surgery, type of neuromuscular blockade used, and body temperature at EOS, did not show a statistically significant association with the PET in multivariate logistic regression.
Table 4 Bivariate and multivariate logistic regression model to identify factors associated with PET among elective adult patients operated under GATE at JMC (N = 308) Jimma, Ethiopia, 2024Older than or equal to 55-year-old patients had six times higher likelihood of having prolonged extubation (AOR = 5.7, 95% CI [2.62, 12.69]). Obese patients (≥ 30 kg/m2) were more than six times more likely to have PET (AOR = 6.6, 95% CI [2.37, 18.36]). The odds of having PET were more than four times higher among patients who have ASA physical status III compared to patients with ASAPS ≤ II (AOR 3.34, 95% CI [1.26, 8.80]). Patients treated with higher academic rank anesthesia providers are less likely to develop (AOR = 0.37, 95% CI [0.15, 0.93], p = 0.035, MSc) and (AOR = 0.25, 95% CI [0.07, 0.55], p = 0.002, anesthesiologist resident (2 and 3). The odds of having PET were 3.4 times higher in those who took BDZ compared to those who did not (AOR 3.42 [1.42, 8.25]). Similarly, the odds of having PET were 0.35 times lower among patients maintained with the isoflurane group when compared to those maintained with halothane (AOR = 0.35, 95% CI [0.15, 0.78]). Patients who underwent procedures lasting more than 2 and half hours had a five times higher probability of developing PET (AOR = 5.2, 95% CI [2.32, 11.72]), and patients who were operated in the prone position had a 4.6 times higher probability of developing PET than those operated in the supine position (AOR = 4.68, 95% CI [1.56, 4.07]). The odds of having PET were nearly threefold higher among patients who were extubated in the afternoon compared to those who were extubated in the morning (AOR 2.67, 95% CI [1.56, 5.74]) (Table 4).
Comments (0)