
Remember me
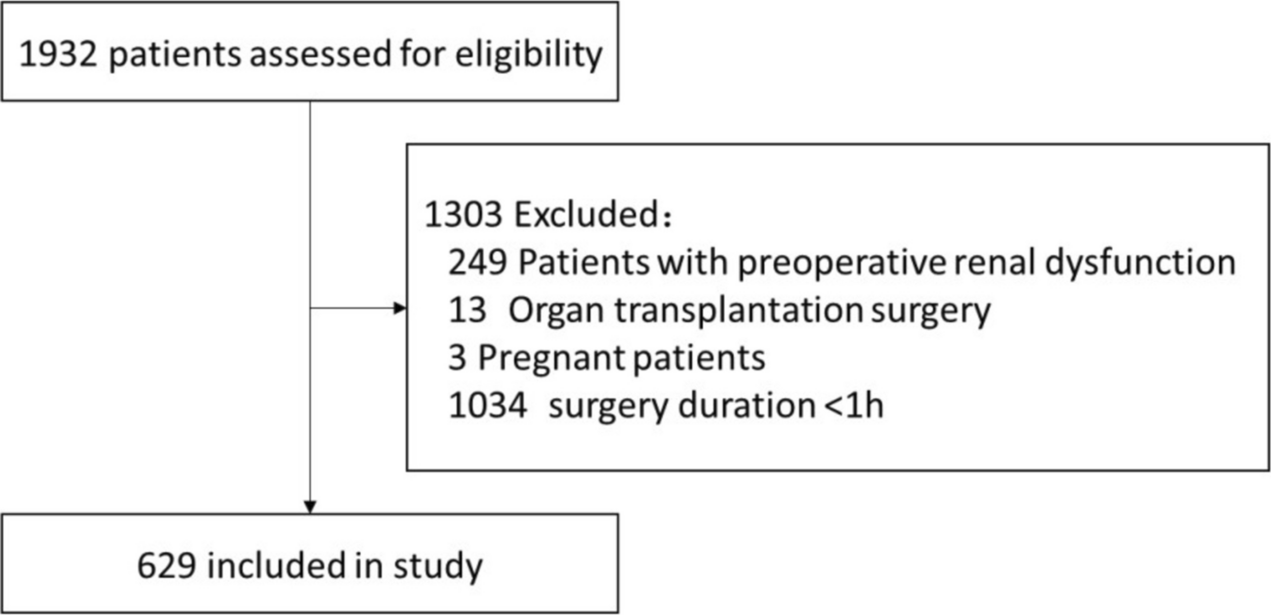

A total of 669 patients were included in the final retrospective analysis. All surgeries between 31/10/19 and 31/12/21 that required a full or mini sternotomy were included. We included patients who underwent elective or urgent surgery but excluded those who underwent emergency surgery. The surgery types were limited to coronary artery bypass (CABG), valve surgery or combined CABG and valve surgery. The mean duration of follow-up was 884 days (range 519–1326). The baseline characteristics of the patients are shown in Table 2.
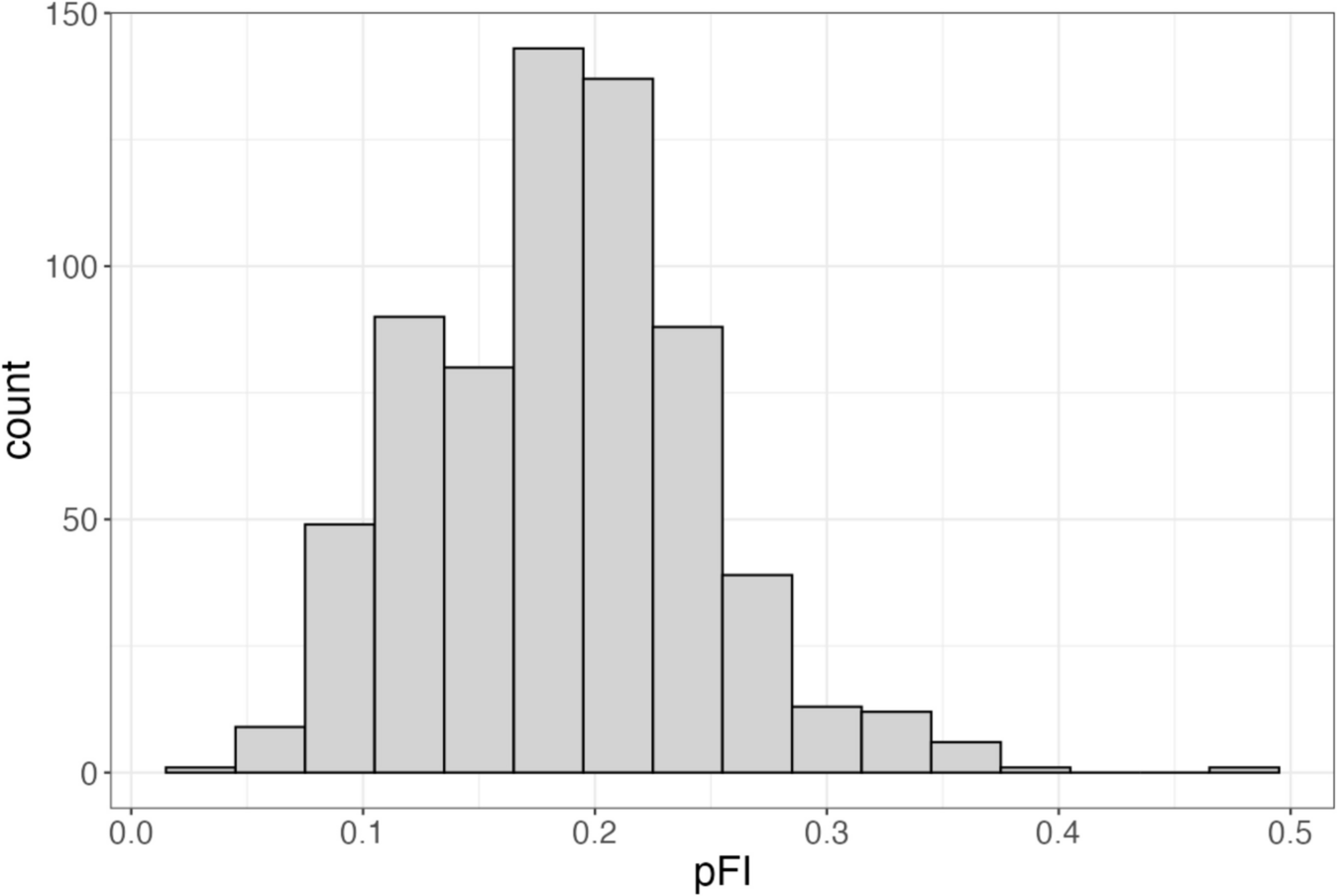
Table 2 Baseline characteristics by binary frailty status (n = 669)The distribution of the calculated pFI score is shown in Fig. 1. The mean pFI score was 0.19 (0.06). A total of 224 (33%) patients were deemed ‘frail’ with a pFI ≥ 0.21, according to the definition applied in a previous large cardiac surgery cohort (McIsaac et al. 2021).
Fig. 1
Histogram of pFI in the cohort of 669 patients undergoing cardiac surgery
‘Frailty’ was associated with a wide range of preoperative comorbidities, as shown in Table 2. The incidence of non-sinus rhythm, chronic obstructive pulmonary disease, heart failure diabetes, a previous myocardial infarction and peripheral vascular disease were all higher in patients living with frailty.
Frailty was strongly associated with being in the lowest decile for deprivation and, to a lesser degree, with deep poverty and deep-rooted deprivation. Notably, frailty was not associated with either sex or advanced age (whether analysed as a binary outcome (age > 70 years) or as a continuous variable (Mann‒Whitney U)).
An ANOVA revealed a significant effect (p = 0.005) of frailty on the duration of intensive care stay and level 3 support, with post hoc tests indicating patients living with frailty spent an extra day longer in intensive care (‘frail’ patients [4.92 (7.82), 95% CI: (3.89, 5.95)] versus ‘non frail’ patients [3.45 (4.63), 95% CI: (3.02, 3.88)]). Patients living with frailty also required level 3 cardiovascular and respiratory support for longer periods (Table 3).
Table 3 Association of frailty with short- and long-term outcomesSignificant differences were found in hospital length of stay (p < 0.001), with patients living with frailty remaining in the hospital longer [13.3 (14.3), (11.4, 15.2)] than ‘non frail’ patients [8.8 (6.51), (8.21, 9.42)].
At 30 days after surgery, the mean days alive and out of hospital (DAOH30) was 19.2 (7.68), and the median was 23 days (interquartile range [IQR], 18–24) (Table 3). ANOVA revealed a significant effect (p < 0.001), with post hoc tests indicating that ‘frail’ patients spent 3 days less at home in the first 30 days [17.2 (8.69), (16.2, 18.2)] than ‘non frail’ patients [20.3 (6.90), (19.6, 21.0)] (Fig. 2). Without adjustment, each 10% increase in the pFI was associated with a 23% (95% CI, 15–30%; p < 0.001) relative decrease in DAOH30. The number of days at home in the first year after surgery (DAH365) was also strongly correlated with the frailty index. Each 10% increase in the pFI was associated with a 10% (95% CI, 2.7–18%; p = 0.008) relative decrease in the DAH365.
Fig. 2
Marginal means plot with 95% CI of days alive and out of hospital in the first 30 days (DAOH30) after cardiac surgery, depending on frailty status
In the first 30 days after surgery, the major mediator of people living with frailty having fewer days at home was time requiring cardiovascular support (68.5%). In addition, there were additional days requiring noncardiac care (4.2%), readmission (3.0%), delayed discharge (3.8%) and 30-day mortality (7.1%). At 365 days, mortality (70.4%) was the major mediator of the reduced number of days at home in ‘frail’ patients. In the full cohort, mortality accounted for 47.5%, and readmission accounted for 22.4%, of reduced days at home in the first year (Table 4).
Table 4 Mediators of reduced DAOH30 (a) and DAH365 (b), in the full cohort and in patients living with frailtyNeither 30-day mortality (frail 1.8%, not frail 2.2%) nor 1-year mortality (‘frail’ 5.4%, ‘non frail’ 4.5%) was significantly associated with frailty.
Survival curves with a median follow-up of 884 days (range 519–1326) for the continuous explanatory variable pFI, with a calculated cut-off of 0.17, revealed a significant association between a high frailty index and the hazard ratio for death, where every 0.1 unit increase in pFI increased the hazard 28 times (0.6–1323, p = 0.004) (Fig. 3).
Fig. 3
Survival curve with a median follow-up of 884 days (range 519–1326) for the continuous explanatory variable pFI, with a calculated cut-off of 0.17
A multiple regression analysis was conducted to assess whether the WIMD modified the effect of frailty on recovery after cardiac surgery. The interaction term (pFI × WIMD) for DAOH30 was not statistically significant (estimate = 9.77 × 10−4, 95% CI [− 0.0176, 0.0196], p = 0.92). Nor was it significant for DAH365 (estimate = 0.0244, 95% CI [− 0.136, 0.184], p = 0.765), indicating no evidence of moderation. Variance inflation factors (VIF) suggested no collinearity concerns (all \(\approx\) 1, except the socioeconomic frailty component = 3). These findings suggest that socioeconomic deprivation does not significantly alter the relationship between frailty and functional recovery after cardiac surgery.
Comments (0)