
Remember me
The search strategy yielded 4428 articles of which 366 were identified as duplicate records, resulting in 4062 unique articles, including original studies and review articles. An additional filter of keywords (see addendum 3 to the protocol) excluded a further 3316 articles.
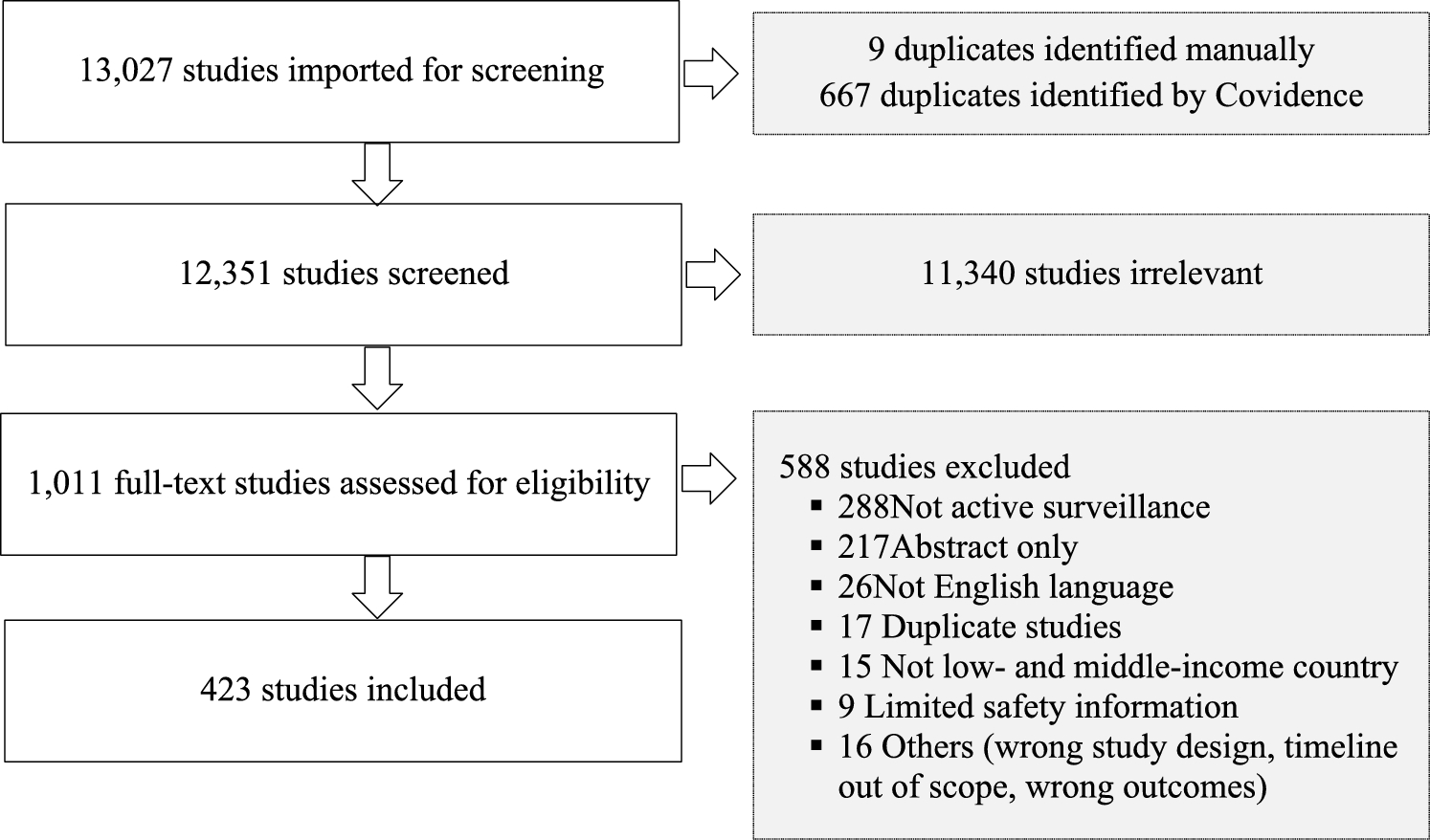
A total of 746 unique abstracts were screened and 37 reports were eligible for full-text review; of these 23 were deemed eligible (see PRISMA flowchart, Fig. 1). Articles were excluded primarily based on the following reasons: studies with no information on follow-up (51%; n = 362), for example, disproportionality analyses, retrospective cohort analyses, case-series reviews, review articles not relating to follow-up (14%; n = 99), or methods research unrelated to follow-up (9%; n = 66).
Fig. 1
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram used to select papers for the scoping review. *Duplicate records between PubMed and Embase were eliminated with Rayyan. **Articles excluded based on keyword search using Rayyan®
3.1 Definition of Follow-Up Within Regulations and GuidanceThe websites of Regulatory/ Health Authorities were reviewed for 37 countries and two regions (The European Medicines Agency (EMA)] [18] and the Caribbean Public Health Agency (CARPHA) [22] in addition to two international guidances (ICH E2D [23] and CIOMS Working Group V; Current Challenges in Pharmacovigilance: Pragmatic Approaches [24]). A detailed overview of the regulations reviewed is included in OSM Table 1.
The CIOMS Working Group V (CIOMS V) [24] and ICH E2D [23] defines “follow-up” as the systematic process of obtaining additional information regarding a reported AE or clinical case after the initial report. ICH E2D notes attempts should be made to obtain follow-up information on as many items as are pertinent to the case and provides an extensive list of possible information attributes including patient details, suspect and concomitant medications, details of the AE, and details of the reporter. Whilst CIOMS provides a similar list, it is stratified into four categories to guide data collection and prioritization based on different ICSR attributes, the CIOMS guidance recommends one follow-up attempt for non-serious expected ICSRs and two for others. Follow-up may be conducted through various mechanisms including written correspondence, telephone calls, or site visits. The CIOMS guidance provides recommendations on prioritizing follow-up, particularly for serious unexpected cases, and suggests conducting follow-up twice: an initial request followed by a subsequent reminder.
The guidelines of an additional 18 regulatory authorities (see OSM Table 1) include some information on follow-up; however, further detailed guidance is provided by a smaller subset (n = 12) (see Table 1).
Table 1 Summary of screening process for regulationsThe range of definitions includes standard requirements to follow-up, which refers to the need to establish routine processes for ensuring follow-up is incorporated into AE management practices. Additionally, some include prescriptive guidance on the mechanism or when follow-up should be conducted including the need for ad hoc follow-up occurring in response to specific conditions being met (e.g., pregnancy) requiring immediate or focused attention. Lastly, risk-based follow-up aims to differentiate AE reports to focus resource on case types that are most likely to impact benefit-risk; currently these include prioritization based on case attributes, for example, seriousness and event labelling.
3.2 Current Legislative Requirements for Follow-UpFor countries or regional guidance in which detailed guidance on follow-up is provided (n = 10; Australia, Canada, EMA, United Kingdom, Netherlands, Pakistan, Saudi Arabia, New Zealand, Malaysia, and Nigeria), legislative requirements for follow-up align with the guidance of CIOMS V and ICH E2D; however, they often take into consideration the local healthcare infrastructure and regulatory maturity. For instance, the EMA and those that incorporate good PV practices comparable to that of the EMA, for example, the UK, Saudi Arabia, and Nigeria, that detail comprehensive follow-up protocols that prioritize the collection of complete, clinically relevant information. Canadian regulations emphasize the need for continued follow-up based on the health professional’s judgement ensuring follow-up is conducted until such a time that an outcome is established. A detailed overview of the regulations reviewed is included in OSM Table 1.
Australia and New Zealand, while less detailed in procedural aspects, underscore the importance of a risk-based approach applied to the follow-up process, whilst Malaysia and Pakistan advocate for continuous information gathering until a case reaches resolution or no further follow-up is possible, emphasizing the need for ongoing PV effort.
In some countries, such as Ghana, Rwanda, Sierra Leone, and Zimbabwe, the focus is on the collection of information constituting a valid ICSR (a minimum number of data fields to be completed), where detailed initial information may be scarce and AE monitoring frameworks are enhancing. Nigeria and Sri Lanka have updated their guidelines in 2021 and 2019, respectively, to establish more structured follow-up protocols aligning to CIOMS V, indicative of an evolving PV landscape that seeks to standardize and enhance drug safety monitoring practices in line with international guidance.
Overall, the variations in follow-up practices not only reflect the maturity and capabilities of national regulatory frameworks, but also significantly influence the global effectiveness of PV systems, underscoring the need for tailored approaches to follow-up based on the maturity of the PV system within a country. However, overall there is limited guidance available within regulations regarding best practices for follow-up procedures. A detailed overview of the regulations reviewed is included in OSM Table 1.
3.3 Follow-Up Methods, Tools, and ValueThe analysis of studies undertaken hereafter is based on the 23 studies that met our inclusion criteria. The studies meeting inclusion criteria were conducted in different settings, such as registries, observational studies, spontaneous reporting systems, and cohort monitoring, and by different stakeholders, including PV centers, MAHs, and academic centers (including hospital-based settings). These studies are summarized in Table 2 and detailed further in OSM Table 2.
Table 2 Summary of included studies stratified by follow-up method3.3.1 Follow-Up Methods and ToolsOf the 23 studies shown in Table 2, five were categorized as utilizing digital communication tools, four as using telephone-based follow-up, three as utilizing electronic medical records or directly engaging with HCPs, two as using active surveillance via home visits, and two in which the method of follow-up was not reported. The remaining seven studies related to methods studies (three utilizing spontaneous reporting systems, one assessing techniques in community-based monitoring, one as a technological aid to guide long-term follow-up, one engaging patients in healthcare forums, and one comparing the value of communications methods in a pregnancy surveillance program).
A summary of results is provided in Fig. 2 showing the distribution of studies by region, initiators of follow-up activities, methods used, nature of follow-up, country of study, and year of study.
Fig. 2
Summary of results on follow-up in pharmacovigilance, showing the distribution of studies by region, initiators of follow-up activities, methods used, nature of follow-up, country of study, and year of study
Initiation of follow-up activities: Follow-up activities were initiated by different stakeholders, including regional PV centers (n = 10), marketing authorization holders (MAHs; n = 6), and academia (n = 7; including hospital-based settings).
Digital communication tools: Five studies [25,26,27,28,29] utilized digital connection tools such emails, online surveys, or SMS to provide reminders for reporting both primary events following administration and subsequent follow-up information. The highest rate of response 100% was observed in the study of Nardone et al. [28], who assessed pediatric nephrogenic systemic fibrosis, the purpose of follow-up in this study was to support de-duplication of cases for a rare event and was undertaken by contacting authors of case reports in publications; in this study all authors responded to requests for further information (n = 8). High response rates (> 70%) for follow-up were also observed for three other studies, and in two of these studies [25, 26] the purpose of follow-up was to monitor AEs post immunization; in this setting response rates were 71.8% and 87%, respectively, and in the remaining study of Kheloufi et al. [27] the study was conducted by a regional PV center in France who assessed if the overall informativeness of initial AE reports could be improved upon if follow-up based. The PV center used predominantly email and telephone as the method of follow-up and noted that in 90% of reports the informativeness improved; they defined informativeness as key pieces of information needed to assess the AE report. The remaining study by De Serres et al. [29] had lower response rates; the study was undertaken within a routine vaccination setting with patients who received the meningococcal B vaccine and were asked to participate in an active surveillance program. In this setting response rates for questionnaires were reported as 31% after the first dose, and 29% after the second dose.
Telephone follow-ups: Telephone interviews were notably effective in four studies needing detailed individual responses, with response rates ranging from 62 [30] to 89% [31] . The highest response rate was observed in a Danish study based on a national register which assessed the long-term psychiatric effects of mefloquine [31]; 89% (76/85 of patients responded to an online survey). Similar response rates (84% [32, 33]) were observed in an active monitoring program to assess the safety of ophthalmic solutions in Peru. In the remaining study follow-up was used to assesses the impact the quality of life of patients who had experienced myocarditis following mRNA COVID-19 vaccination in the USA, and achieved a 62% response rate [30]. Successful follow-up in these studies was defined as the completion of either a follow-up survey or questionnaire to which the patient responded.
Healthcare provider/use of medical records: The direct involvement of healthcare providers or access to medical records were utilized in three studies [34,35,36] to supplement collection of additional data following initial reporting of an AE. Moro et al. [34] utilized VAERs and subsequently requested medical records for outcome information on pregnant women who received the Influenza A (H1N1) 2009 Live Attenuated Monovalent Vaccine receiving 84% of records (95/113), although the study did not specify how the medical records were obtained. Filippi-Arriaga et al. [35] monitored unlisted events within a hospital setting and successfully followed up using EHRs for all patients to assess the likelihood of causality. The remaining study, by Chen et al. [36], was an active post-marketing PV program to monitor events of interstitial lung disease associated with abemaciclib through structured questionnaires and interviews directed to the HCPs, although specific performance was not reported for this study.
Active surveillance via home visits: Two studies involved the use of home visits; both studies were cohort-monitoring studies associated with the use of antiretrovirals [37] and antimalarials [34], where follow-up was conducted to support active monitoring of AEs. The study of Dodoo et al. [38] noted that home visits were essential for direct patient interaction, ensuring data collection continuity in less technologically advanced rural settings within Ghana; this method proved particularly effective where a 74% follow-up rate was achieved. The study of Mussa et al. [37] conducted in Mozambique did not provide a quantification of response rates but utilized a mixed method of routine home visits and telephone calls to support active monitoring. The methods for these studies did not confirm if any feedback or additional information was provided to patients relating to the AE.
Follow-up mechanism not reported: Two studies did not report the mechanism by which follow-up was undertaken, Marshall et al. [40] noted that 88% of patients responded to information requests for event outcomes following vaccination with meningococcal B vaccine. Whilst De Vries et al. [39] collected pregnancy-related information utilizing a questionnaire (mechanism of delivery not described) for patients administered adjuvanted A/H1N1 (2009) influenza vaccination within a prospective cohort, the authors noted a response rate of 95% (281/295 pregnant females) was observed. The authors in this study attributed the high response rate for follow-up likely due to enrolling patients in the last trimester of pregnancy.
3.3.2 Nature of Additional Follow-UpOf the 16 non-method-based studies, five focused on follow-up of specific AEs including myocarditis [30], long-term psychiatric effects [31], and interstitial lung disease [36] or outcomes, and pregnancy following vaccine administration [34, 39]. Eight studies focused on open-ended follow-up of AEs post administration, and the intent of the remaining three studies was to support deduplication [28], improve the informativeness of an AE report [27], and characterize the seriousness of unlisted ADRs [35].
Follow-up of a specific AE or outcome: Kracalik et al. [30] assessed the impact of myocarditis on quality of life following mRNA COVID-19 vaccination. In their study, follow-up data were collected for 62% of the patients. The follow-up, conducted at least 90 days after the onset of myocarditis, enabled an evaluation of its long-term effects, noting most individuals in the exposed cohort recovered with minimal impact to their quality of life post 90 days.
Ringqvist et al. [31] assessed the long-term psychiatric effects of mefloquine via a national register using bespoke psychiatric surveys to assess the impact on psychiatric health. Follow-up in this study was conducted 988 days (mean) from the occurrence of the event, which enabled the authors to conclude there remained long-term psychiatric effects of mefloquine compared to the control group.
Chen et al. [36] utilized targeted follow-up questionnaires and interviews for spontaneously reported AEs of interstitial lung disease; follow-up was conducted for a period of 6 months following AE occurrence. Through the assessment of data collected, the authors were able to assess potential risk factors contributing to the development of fatal outcomes.
Moro et al. [34] and De Vries et al. [39] aimed to characterize maternal and infant outcomes for pregnant women who received an influenza vaccine. The follow-ups in these studies were conducted to obtain pregnancy outcome and infant data from medical records up to 6 months of age [34] for Moro et al., and 6 weeks after the estimated date of birth for De Vries et al.
Open ended follow-up post administration: Open-ended follow-up in this context refers to follow-up undertaken with no pre-determined AE, but rather open-ended to support active safety monitoring post drug or vaccine administration. Eight studies focused on open-ended follow-up of AEs post administration. Of these, four [25, 26, 29, 40] were conducted with vaccines in which patients had consented to be included within a registry or monitoring system. The intent of these studies was to monitor post-vaccination safety where patients experiencing AEs were followed up for outcomes and severity to inform on the overall safety profile. In one study the authors noted the outcomes helped increase confidence to support vaccine uptake [26], whilst in another follow-up via medical records led to the identification of nephrotic syndrome [29], a rare event indicative of severe renal disease which required further investigation. The monitoring period in these studies ranged from 4 months to 1 year.
Four studies focused on open-ended follow-up of AEs post drug administration for antimalarials [38] and anti-retrovirals [37], and two related to ophthalmic products [32, 33]. In two studies [37, 38] patients were consented to participate within a monitoring cohort where patients were contacted periodically via home visits to assess overall safety in the target population. In two studies [32, 33] follow-up was undertaken via spontaneous reports; where ICSRs were followed up 30 days apart via telephone calls, the intent of monitoring and subsequent follow-up were to inform on the severity, seriousness, and any associated sequalae associated with the AE experienced.
Other reasons for follow-up: In the remaining three studies the intent of was to support deduplication [28], improve the informativeness of an AE report [27], and characterize the seriousness of unlisted ADRs [35]. In the first study Nardone et al. [28] aimed to collate AE reports for rare pediatric nephrogenic systemic fibrosis cases across multiple databases, the intent of follow-up in this study was to enhance case deduplication for a rare event.
In the second, Kheloufi et al. [27] conducted a study to describe the informativeness of AE reporting in France and estimate the contribution of a review by a PV assessor on the informativeness of these reports, pre and post follow-up; they noted contacting the reporter for follow-up increased the informativeness of the report for more than 90% of reports. The study does not highlight how soon after AE reporting individuals were contacted.
The remaining study, by Filippi-Arriaga et al. [35], aimed to characterize the seriousness and outcome of unlisted ADRs at the time of report and at follow-up within a hospital setting. The follow-up period was defined from the date the drug-event pair was identified until the date it was resolved or a maximum of 1 year after the report. During the follow-up period, pending or new results from laboratory tests, imaging studies, biopsies and skin tests were reviewed. Based on the results and the medical criteria of the evaluator, it was determined whether these complementary tests helped to reinforce the causality of the drug-event pair or to diagnose alternative causes.
Impact of follow-up for pre-consented versus spontaneously reported AEs: Of the 16 studies reviewed, seven included pre-consented patients who were periodically followed up at defined intervals. In these studies, response rates for follow-up varied widely, ranging from 31 [29] to 95% [39]. The remaining nine included studies where follow-up was conducted without prior consent to be contacted; of these, five were conducted using spontaneous reporting databases with follow-up performance ranging from 84 [32,33,34] to 90% [27]; one study did not report follow-up performance [36]. Among the remaining four studies, two utilized national registers [31] or were conducted by a national PV center [30], one employed retrospective medical records for follow-up [35], and the last study aimed to support deduplication efforts [28].
3.3.3 Studies Evaluating Follow-Up MethodsSeven studies evaluated follow-up methods or provided performance assessments of current SRS systems; three of the studies were conducted within safety databases. Vemula et al. [41] described the overall performance of the Novartis PV system as it relates to follow-up, noting that 32% and 19% of reports successfully receive follow-up for attempts 1 and 2, respectively, therefore advocating for a risk-based approach to follow-up. This was demonstrated by Geissbühler et al. [43], where Novartis via the Pregnancy outcomes Intensive Monitoring (PRIM) undertake multiple attempts (n = 4) at follow-up of pregnancy reports, but the performance of this approach was not reported. Laemmle et al. [42] shared lessons learnt following the COVID-19 pandemic demonstrating how safety systems were deployed which integrate with immunization provider management software to issue automated surveys; however, the performance was not reported.
Two studies were methods comparison studies aiming to compare current practice to an active follow-up program [
Comments (0)