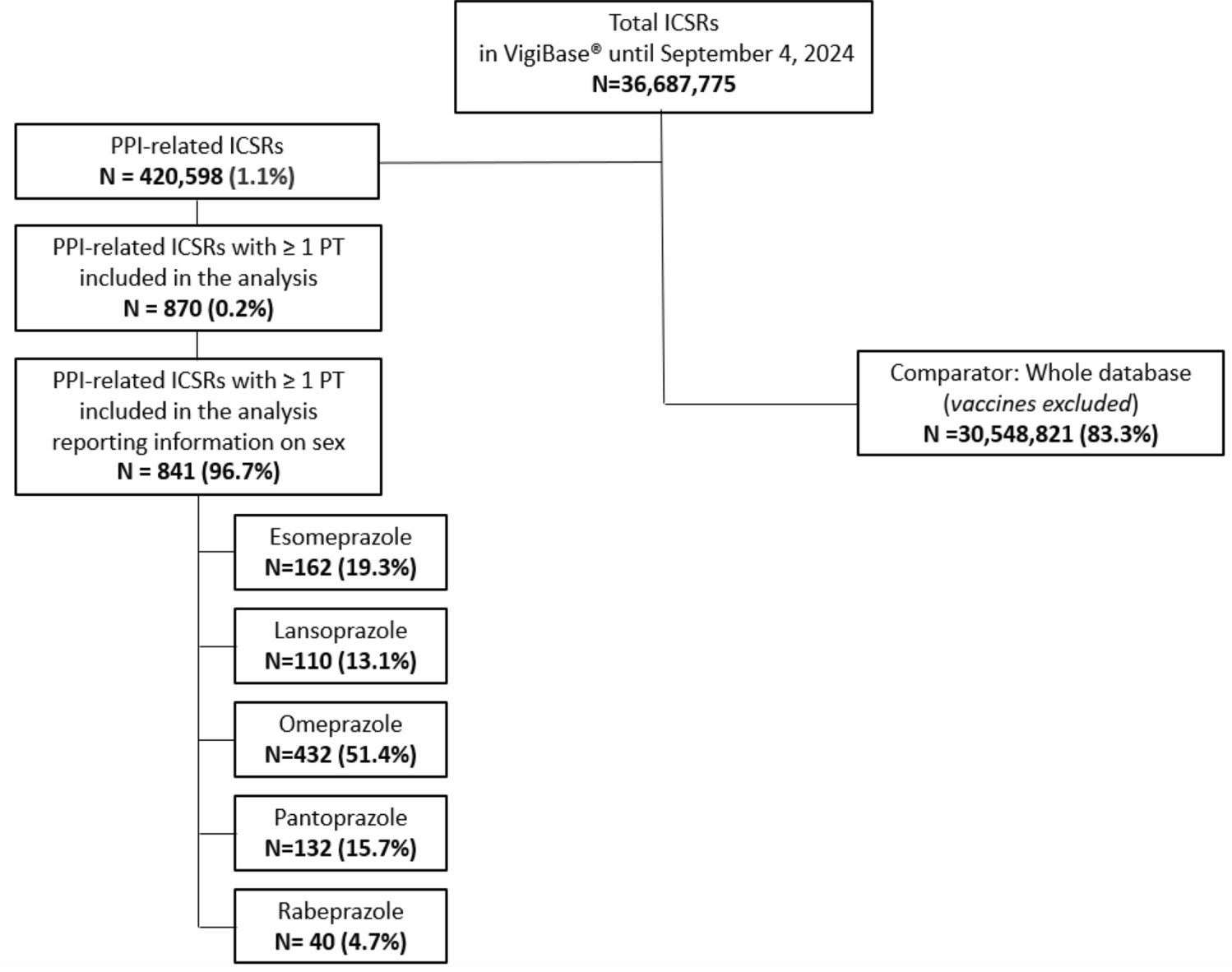
To the best of our knowledge, this is the first pharmacovigilance study using VigiBase to investigate the potential role of PPIs in inducing SDs in both male and female patients. We found potential safety signals for omeprazole-induced ED in male patients, and esomeprazole-induced genital discomfort and oestrogen deficiency in female patients. Findings for the subgroup analysis restricting the study population to patients aged from 18 to 64 years also showed additional potential safety signals concerning an omeprazole-induced libido decrease and esomeprazole-induced hypogonadism in male individuals, as well as omeprazole-induced genital discomfort in female individuals. Although spontaneous reporting systems do not allow for the estimation of incidence rates of ADRs, the relative frequency of reports may still provide an approximate indication of the potential magnitude of the problem. In this regard, the finding that only 0.2% of ICSRs involving PPIs referred to SDs does not reflect the true incidence of these events, but it may nevertheless suggest that such reactions represent a relatively uncommon or unknown, yet clinically relevant, safety concern.
It has been estimated that about 25% of all cases of ED are caused by medications, especially antidepressants, antipsychotic drugss, antihypertensive medications, antineoplastic medications, antihistamines, drugs with anticholinergic activity and anti-hormones [31, 32]. The prevalence of iatrogenic ED could be even higher considering that several non-communicable chronic diseases share the ability to produce SDs through the same proinflammatory mechanism of action, but are, at the same time, treated with a number of the above-mentioned erectolytic drugs [33].
While blockers of the type 2 histamine receptor, used for the treatment of gastric hyperacidity, are well known to produce SDs through an anti-histaminergic effect [6], the current medical literature evaluating the association between PPI use and ED onset is limited. One of the first studies exploring the potential association between ED and omeprazole was a pharmacovigilance study conducted by the Uppsala Monitoring Center, dating back to 1992 [7]. This study described 15 cases of ED potentially associated with omeprazole use, including two cases involving men under the age of 40 years [7]. More recently, in 2015, pharmacovigilance reports published by Lareb suggested a potential association between ED and omeprazole or lansoprazole, with a latency period that ranges from 1 day to 6 months [5]. Such evidence is in line with our findings, as we observed a median TTO for potential omeprazole-induced ED of 19 days with an interquartile range from 4 to 180 days. The latency period observed between PPI initiation and the occurrence of SDs appears consistent with a plausible causality, as SDs may emerge relatively early during therapy. This pattern contrasts with other adverse events potentially associated with long-term PPI use, such as nutritional deficiencies or bone fractures, which typically require prolonged exposure before becoming clinically evident. Supporting such evidence, a case report published in 2021 documented the sudden onset of severe ED in a healthy young man shortly after starting over-the-counter omeprazole therapy. The patient’s erectile function rapidly returned to normal following the discontinuation of the drug [8].
In recent years, regulatory agencies including the EMA [11], the FDA [34], and the Malaysian National Pharmaceutical Regulatory Agency [35] have issued safety notifications regarding the potentially increased risk of ED in patients receiving PPIs.
Following an analysis of the FDA Adverse Events Reporting System in 2022, the FDA acknowledged ED as a potential safety signal associated with PPIs [36]. As a result, in 2023, this regulatory agency determined that the SmPCs for all PPI-containing products, including combination products and combination packs, must include information about the risk of ED onset [37]. However, to date, the risk of ED is not mentioned in the EMA SmPCs of PPIs. Additionally, the esomeprazole periodic safety update report single assessment (PSUSA/00001269/202403) issued by the EMA Pharmacovigilance Risk Assessment Committee at the end of March 2025 did not mention any association between esomeprazole and ED [37].
Concerning the aetiopathology of PPI-induced ED, several mechanisms have been suggested in the literature. One of these is the induction of the cytochrome P450 3A4 enzyme by PPIs, which may reduce testosterone levels in some patients, thus leading to low desire and subsequent ED. Another pathological pathway may involve the ability of PPIs to impair endothelial nitric oxide production, which plays a role in in cavernous smooth muscle relaxation and finally in erectile function, thereby leading to ED [38, 39].
After testosterone, prolactin is considered one of the most important hormones affecting male sexual function [40]. Prolactin acts negatively on erectile function through central and peripheral mechanisms not fully understood [12]. In fact, dopamine is regarded as a major factor in triggering sexual motivation [13], implying that an enhanced dopamine level in the brain regions related to reward would lead to increased sexual drive [14]. At the same time, dopamine controls and reduces the lactotroph activity [15]. In this regard, peripheral high levels of prolactin reflect a central reduction of the dopaminergic pathway [12]. This has not been yet demonstrated as a possible mechanism of action of PPI-induced hyperprolactinemia. This lack of evidence jeopardises a clear-cut explanation of the sexual symptoms found in patients treated with PPIs long term. In fact, direct effects of prolactin on the sexual behavior have been demonstrated only in the above-mentioned peripheral inhibition of the nitric oxide synthase activity, while the anti-sexual effects of hyperprolactinemic drugs have been consistently referred to their antidopaminergic activity, as happens with antipsychotic drugs [16]. Hence, if PPIs do not directly reduce dopamine central activity, prolactin may do it [17], partially explaining the sexual dysfunctions here discussed. However, the circularity of these loops remains to be fully elucidated.
Although the findings of our study did not show statistically significant disproportionality for PPI-induced hyperprolactinemia, safety signals generated by our analyses concerning oestrogen deficiency, libido decrease and hypogonadism might be explained by increased prolactin levels due to PPIs. In particular, two cross-sectional studies investigated the role of prolactin in the onset of PPI-related SDs in male and female patients, respectively. The first study involved 65 male patients consistently receiving PPIs for at least 3 months and showed significant variations for decreased libido, ED, and decreased semen volume between normal and hyperprolactinemic PPI users [18]. In another cross-sectional study of 101 patients receiving PPIs for at least 3 months, significant hormonal changes were observed in those who reported sexual complaints. These patients had significantly different levels of prolactin, oestrogen and progesterone compared with those without such problems. This study also found a statistically significant increase in the incidence of amenorrhea, menstrual irregularities, breast enlargement and breast tenderness in patients with elevated prolactin levels [41].
Proton pump inhibitor-induced SDs may also stem from other indirect mechanisms. Proton pump inhibitors have been found to disrupt the absorption of vitamin B12 and magnesium [42, 43], deficiency of which are suspected to be contributing causes of SDs and infertility in both men and women [42, 44, 45]. Last, findings from the notoriety analysis highlighted a considerable heterogeneity among EMA and FDA SmPC for the study drugs, confirming the results of previous comparisons [46, 47].
One of the main strengths of this study is that, to the best our knowledge, this is the first to provide an overview of potentially PPI-induced SDs using a spontaneous reporting database. Pharmacovigilance assessments represent an essential and reliable opportunity to monitor drug safety [48]. Spontaneous reporting systems are solid tools to detect and characterise ADRs under real-world conditions, not only for early detection of safety concerns with new drugs, but also for continuous monitoring of old medications [49], thus, supporting the emerging role of pharmacovigilance for risk-benefit assessments [50]. The analyses conducted in VigiBase were supplemented with a thorough review of both EMA and FDA SmPCs of PPIs with statistically significant disproportionate reporting of specific SDs for a notoriety assessment.
However, there are some limitations to acknowledge. First, spontaneous reporting data are generally subject to several biases, including under-reporting, selective reporting and the lack of a denominator (total number of drug users), all of which prevent measuring the absolute risk of suspected ADRs [51]. Second, disproportionality analyses reflect reporting imbalances and are not suitable to evaluate ADR incidence, risk or causality. Third, the absence of causality assessments and the significant lack of relevant clinical information, particularly for ICSRs that generated potential safety signals, represent two major limitations of our analysis. Moreover, the possibility of residual confounding due to factors not fully captured in spontaneous reporting systems cannot be completely ruled out. Fourth, as it was not possible to exclude other drugs known to induce SDs (e.g. antipsychotic drugs, testosterone-5-alpha reductase inhibitors and antidepressants) from the scrutiny, results of a disproportionate analysis may be affected by co-prescription bias (or confounding by association). In fact, it should be considered when evaluating our data that PPIs are not only used to cure gastric and oesophageal symptoms and diseases but also used frequently in association with other drugs known for their ability to attack the gastric mucosa, such as corticosteroid and non-steroid anti-inflammatory drug treatments. These treatments are typically, but not exclusively, used in the elderly. In these cases, polytherapy and the climaterium [52] should be also considered as a further possible risk factors in PPI-induced SD. Nevertheless, it should be considered that only ICSRs reporting PPIs as suspected or interacting drugs were included in the analysis. Fifth, through the descriptive analysis of these ICSRs, we identified potentially differential source patterns for geographical locations and reporters. As an example, while SD- and hyperprolactinemia-related ICSRs were more frequently reported in America than in Europe, ICSRs of lansoprazole-induced SDs, for both male and female patients, were mostly reported in Europe rather than America. As reported by Mestres et al. in 2024 [53], differential source patterns in signal detection could predispose certain drugs to be disproportionally associated with adverse events. Sixth, we conducted disproportionality analyses using both crude and Bonferroni-adjusted RORs. Other disproportionality methods (e.g. proportional reporting ratio, Bayesian Confidence Propagation Neural Network and empirical Bayes geometric mean), which might have contributed to identifying additional PPI-related SD signals, were not applied in this study. Finally, disproportionality analyses do not allow the quantification of the true risk of suspected ADRs, and potential signals detected through the analysis of SRS databases should be validated further. As such, the analysis of SRS is mainly aimed to generate hypotheses, and a causal association between the drugs and the studied ADRs can only be confirmed with patient case reports. Notably, only 0.2% of PPI-related ICSRs in VigiBase were associated with SDs. This finding may suggest that the incidence of SDs related to PPI use is substantially lower compared with other, more commonly reported ADRs.

Comments (0)