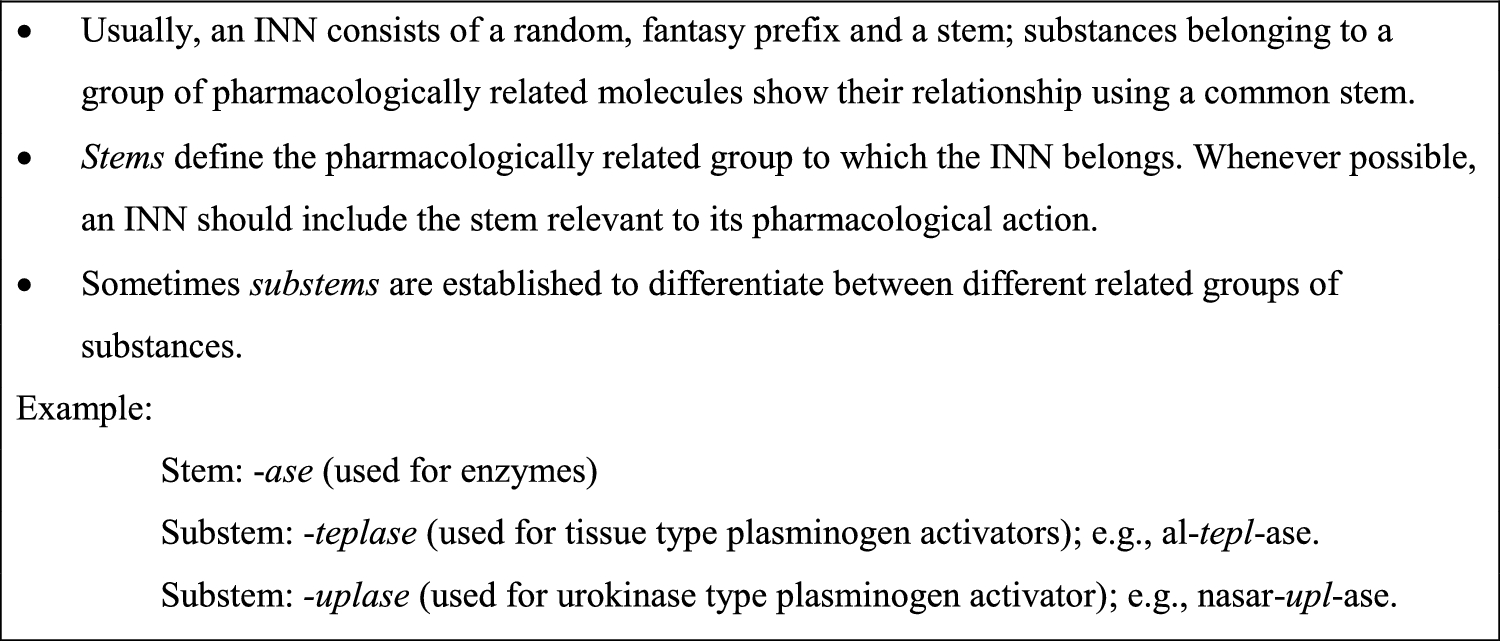
It is not rare for individual drugs within a class to show a unique adverse reaction pattern, slightly different from that of the other stem members, owing to specific molecular characteristics, minor differences in metabolic pathways, or known or unexpected interactions with secondary targets that are only discovered during large-scale clinical use of the medicine. These cases are of great interest in post-marketing monitoring, because rapid identification and verification of such signals help refine cautions and contraindications; additionally, in certain cases, these differential ADRs require regulatory actions, such as withdrawal of authorisation because of unacceptable toxicity. Table 1 includes some examples.
Table 1 Examples of medicines that required regulatory actions because of a differentiated risk compared with other substances sharing the same stemCerivastatin represented a unique case within the statin class, illustrating how molecular differences can create distinct safety profiles. While all substances sharing the -statin stem can cause myopathy and rhabdomyolysis, severe muscle toxicity was more frequent with cerivastatin, 3.16 cases of fatal rhabdomyolysis per million prescriptions, unacceptably higher than the 0.19 cases per million seen with other statins. After 52 deaths worldwide were attributed to cerivastatin-induced rhabdomyolysis, it was withdrawn in 2001 [15]
Troglitazone is a compelling example of how subtle molecular differences between substances sharing the same stem can lead to concerns about harms. It belongs to the stem -glitazone (peroxisome proliferator activating receptor-γ (PPAR-γ) agonists, thiazolidinedione derivatives). It was approved in 1997, and it soon became apparent that it had a unique hepatotoxicity profile not seen with other -glitazones, like rosiglitazone and pioglitazone. Troglitazone was withdrawn in 2000 after reports of 90 cases of liver failure, with several deaths or patients requiring liver transplantation, while other members of the stem remained on the market with acceptable patient safety profiles [16].
Efalizumab exemplifies how biologics sharing the same stem and substem (-zumab for humanized monoclonal antibodies) can exhibit unique concerns. While all immunosuppressive biologics carry inherent risks of opportunistic infections, efalizumab posed unprecedented concern, because it was associated with progressive multifocal leukoencephalopathy (PML). Between 2003 and 2009, four confirmed cases of PML emerged among approximately 46,000 treated patients. This risk was noteworthy because PML had not previously been associated with psoriasis treatments. The drug was voluntarily withdrawn from global markets in 2009 [17].
The stem -coxib (selective cyclo-oxygenase inhibitors) is an interesting example that shows how drugs within a stem can have varying degrees of risks for class-related adverse reactions. These drugs were developed and marketed as having a lower gastrointestinal risk than non-selective inhibitors, which is true. These new drugs were therefore promoted among users of non-steroidal anti-inflammatory drugs (NSAIDs), including elderly people. This rapidly increased use of new medicines led to detection of unexpected and serious ADRs that led to the withdrawal of some selective inhibitors and a call to use both selective and non-selective COX inhibitors carefully [18,19,20,21,22].
The stem -oxacin (antibacterials, nalidixic acid derivatives) includes fluoroquinolone antibacterials. Although they have the same mechanism of action, one or more members of the class have different ADRs to others in the class; trovafloxacin was withdrawn from the market because of fatal liver toxicity [23], and grepafloxacin because of serious cardiac arrhythmia [24].
In cases like these, substances have been withdrawn from the market after causing several deaths. In contrast, in other cases, the confirmation of a signal has led to modification of the recommended dosage regimen, including contraindications or advice to avoid certain concomitant treatments.
In contrast, ciclosporin and tacrolimus have different stems, but both are calcineurin inhibitors with immunosuppressant effects and a similar adverse reaction profile. Sirolimus shares its stem with tacrolimus, but it inhibits the mTOR (mammalian target of rapamycin); their safety profile is quite comparable, dominated by the immunosuppressant effects.
Pharmacovigilance aims to learn from these cases and improve detection systems, to accelerate the spotting of unexpected adverse reactions and to prevent as many deaths as possible. The crucial aspect is that a broad knowledge of the shared safety profile of the stem can help to speed up identification of any adverse effects pattern that significantly differs from the expected one.

Comments (0)