This study investigated the effect of oral neuromuscular training with IQoro on decannulation from a cuffed tracheostomy tube and swallowing function, in patients with severe ABI. Results showed that the IQoro group tended to have fewer days until decannulation compared to the usual care group, but the result were not statistically significant. Furthermore, through visual inspection of the Kaplan–Meier graph, it is also apparent that the differences between the two groups in time until decannulation were seen in the period following the 4 weeks intervention. Thus, making it more likely to have been caused by other factors than the intervention, such as differences in consciousness level, cough reflex and strength; along with active infections which are a contraindication of decannulation from a cuffed tracheostomy tube [20, 26].
Surprisingly, it was only the usual care group which improved on the PAS and Yale scale, which describes the risk of aspiration and amount of residue in the vallecula and pyriform sinus, respectively. It is noteworthy that the usual care group had less residue in pyriform sinus following the training protocol, compared with the IQoro group. This result points to a potentially harmful effect of IQoro training in tracheostomized patients. However, this might well be a chance finding due to the low number of participants, and findings needs to be replicated before conclusions may be drawn.
According to the International Classification of Functioning (ICF), swallowing is described as functions including both the oral, pharyngeal and oesophageal processes related to transporting food and drinks [27]. Some of the previous observational studies on IQoro by Hägg and Tibbling [15, 16] related to swallowing difficulties, have investigated the associations between training with IQoro and lip closure and facial functions [15, 16], but also swallowing capacity, which is a more collective process encompassing both the oral and pharyngeal processes of swallowing. More recently, Hägglund et al. [14] carried out a cluster-randomized study in which swallowing rate and aspiration risk was assessed. Decline in aspiration risk was seen in the IQoro group, but not in the control group. However, aspiration risk was based on unblinded subjective assessments based on a water swallowing test, and findings may therefore be biased [14]. In the present study, instrumental assessment of swallowing function was applied, which should provide more valid and objective assessments. Additionally, it should be considered that the intervention in the study by Hägglund et al. [14] was performed in 16 care units, and the usual care was performed in 18 other care units. Since usual care is not described in detail, results in favor of IQoro may also be due to differences in the usual care practice between care units. In the present study, the focus was on the pharyngeal phase of swallowing as the pivotal mechanism of action driving the weaning process from a cuffed tracheostomy tube [12], because it is argued by Hägg and Morris [13] that training with IQoro activates all the muscles in the swallowing process. However, the scientific rationale behind this assumption is ambiguous.
In relation to level of consciousness and cognitive functioning, participants in the study had median RLAS scores of four and five in the IQoro and usual care group at baseline, respectively. Thus, apart from having tracheostomy tube, they are a different patient group than those described in previous research on IQoro, which consist of community dwelling individuals with stroke and elderly individuals in care facilities [15,16,17]. Therefore, the results should be interpreted with caution, since level of consciousness have been associated with time to decannulation [20, 26].
Trained occupational therapists performed IQoro training for most participants in the present study providing more robustness to the training protocol, whereas training seemed to be mostly self-administered in the previous studies [15,16,17]. On the other hand, motivation to participate in the present study may be lower than previous studies, because most participants were not able to consent themselves due to fairly low level of consciousness and cognitive functioning at enrollment. In line with this, agitation was often the cause when IQoro training was not carried out. However, the study was carried out in a hospital setting in which a tight schedule was kept in order to complete the training protocol. Additionally, patients were only enrolled in the study if they could cooperate on mouth closure. Therefore, although motivation may have been less compared with previous studies, the adherence rate with the IQoro training protocol was deemed high on a group level [28].
In recent years there has been a large increase in available medical devices and it is anticipated that the global medical device market size will increase from 542 billion USD in 2024 to 886 billion USD in 2032 [29]. Based on this growth, it is challenging for research to keep up with advertisements for medical devices and consumer demands [30]. IQoro is a medical device which is boldly stated to be a treatment for the underlying cause of both swallowing difficulties, reflux, heartburn, snoring, and sleep apnoea [13, 31]. Based on this premise, IQoro is stated to have been used by more than 100,000 clients [31]. However, the scientific evidence for its effectiveness cannot keep up with the increasing demands. Thus, high-quality studies by research teams with no conflicts of interest is urgently needed for medical devices such as IQoro.
IQoro is not the only oral neuromuscular training device in the market. A cheaper alternative is Muppy®, which works in the similar way as IQoro, although it has been described that it does not produce the same vacuum in the mouth as IQoro [32]. The effect of Muppy on swallowing function have been investigated in a recent RCT including 40 individuals with first-time stroke [32]. A total of 20 participants received usual care for 5 weeks (orofacial-sensory-vibration stimulation), and 20 participants received usual care plus daily training with Muppy. There was no improvements on aspiration risk measured with PAS in neither the intervention or usual care group, and therefore also no between-group differences. Between-group differences in swallowing rate and lip force was seen at 12 months follow-up only, and these results are therefore likely to be due to other reason than the intervention. If IQoro and Muppy will show an effect on dysphagia in future studies, it would be relevant at to compare the effectiveness of IQoro and Muppy on dysphagia.
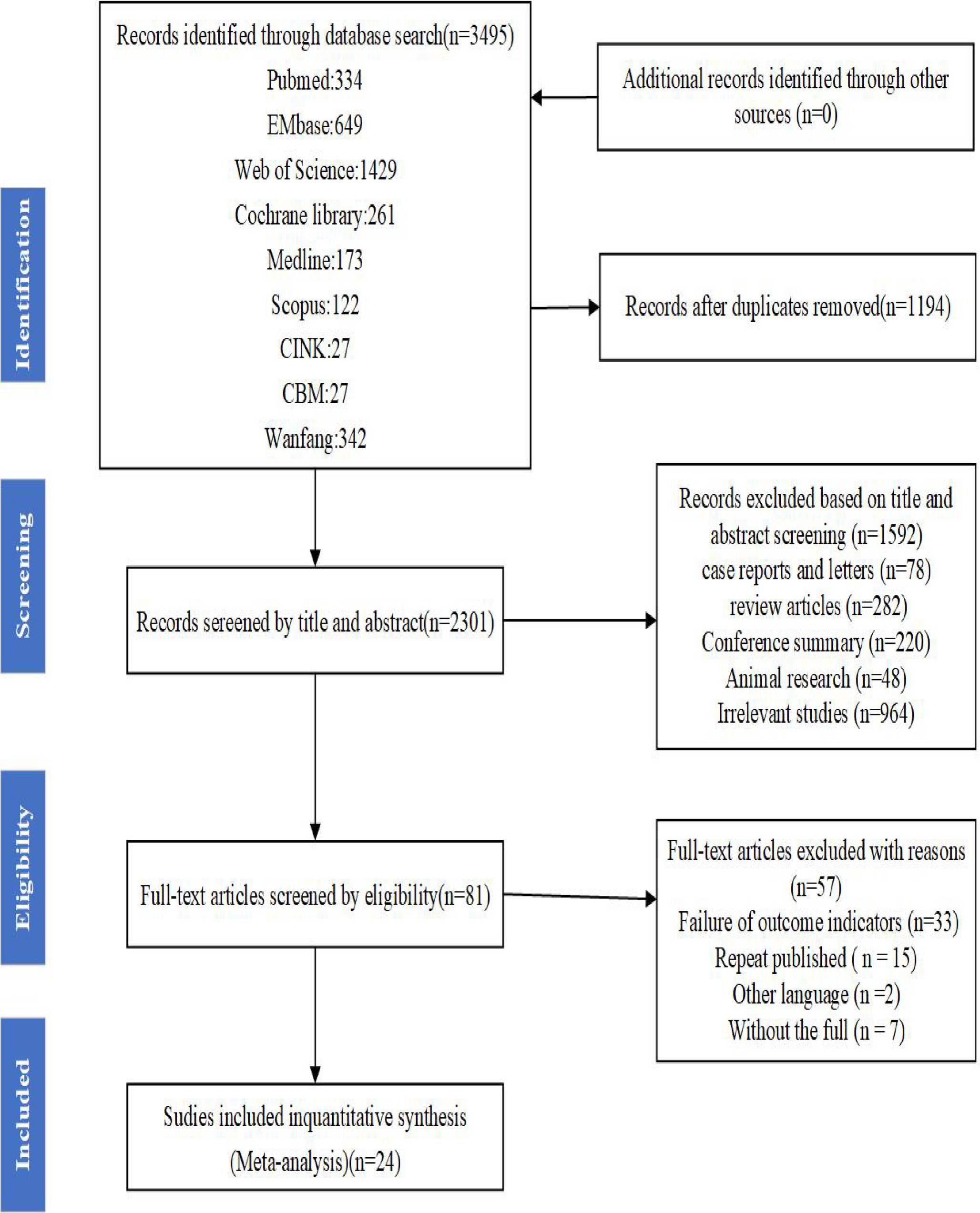
The present study has some strengths and limitations which deserves mentioning. Only 22 participants were enrolled, which was due to a power calculation based on the study by Hägglund et al. [14]. This calculation may be questioned due to potential bias in the study on which it was based, but the calculation was made due to lack of studies with populations and outcomes, which more closely resembled the present study. However, 22 participants fullfilling our inclusion criteria are difficult to come by, which is also illustrated in the flowchart, and also the reason why it took two years to enroll enough participants. It could be seen as a limitation that a very selective population of patients with tracheostomy tubes due to ABI were enrolled, because it limits generalisability of findings. However, it could also be seen as a strength since results show that IQoro may not be suitable for this particular patient category. IQoro was used sporadically for this patient category at the ward before the study, and the intervention is therefore a clear reflection of clinical practice at the ward. This also means that the results are a clear representation of the effect of IQoro in normal clinical practice, outside the frame of a clinical trial. Following the study, clinicians at the ward will now refrain from training swallowing function with IQoro for patients fulfilling the study eligibility criteria.
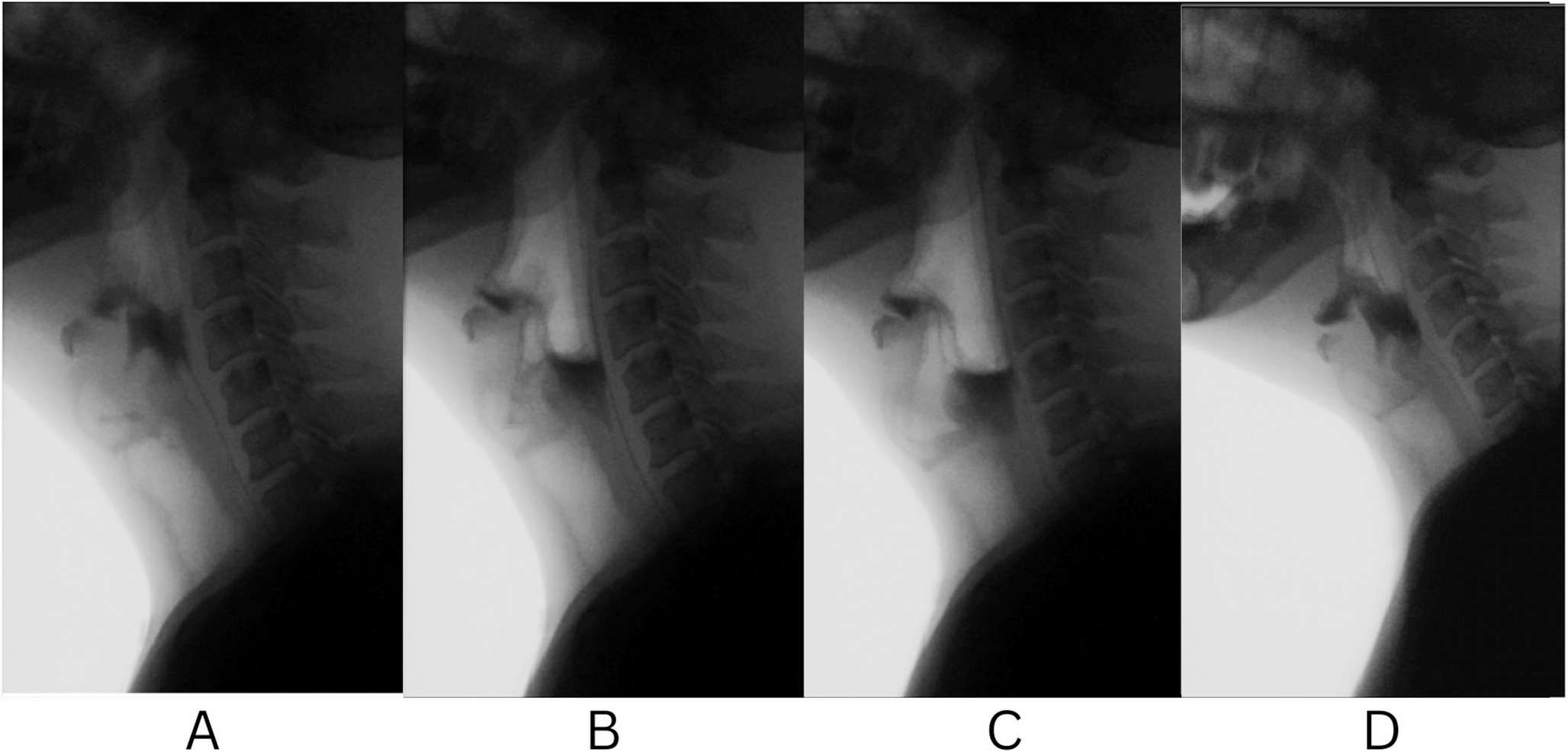
Decannulation and swallowing assessment was not done by assessors who were blinded to treatment allocation due to logistic reasons. However, FEES is a fairly objective assessment of swallowing function, on which decisions on the weaning proces is based, and blinded assessors are therefore not likely to have changed the results of the study. Additionally, it is obvious that it is not possible to blind participants, but since the patients had low consciousness and mostly did not consent to participate by themselves, it is not suspected that placebo and hawthorne effects have played any great role on the results.
Clinical and Research Implications
In this study we found that four weeks of training with an oral neuromuscular training device named IQoro, as an add-on to usual care, was not superior to usual care alone, in improving swallowing function and reducing time until decannulation in patients with severe ABI. On the contrary, findings from the FEES showed a potentially harmful effect of IQoro with less improvements in pharyngeal residue in the IQoro group compared with the usual care group. However, this finding needs to be replicated before any conclusions may be drawn.
The study results should not be generalized to patient categories outside the eligibility criteria, since this is a highly selective population in which injury severity and consciousness level may also have an effect on swallowing function and successful decannulation. Future studies investigating the effect of IQoro and similar training devices on a more general population of non-tracheostomized patients with ABI are warranted, in order to have scientific evidence which can keep up with marketing strategies and consumer demands for products such as IQoro.


Comments (0)