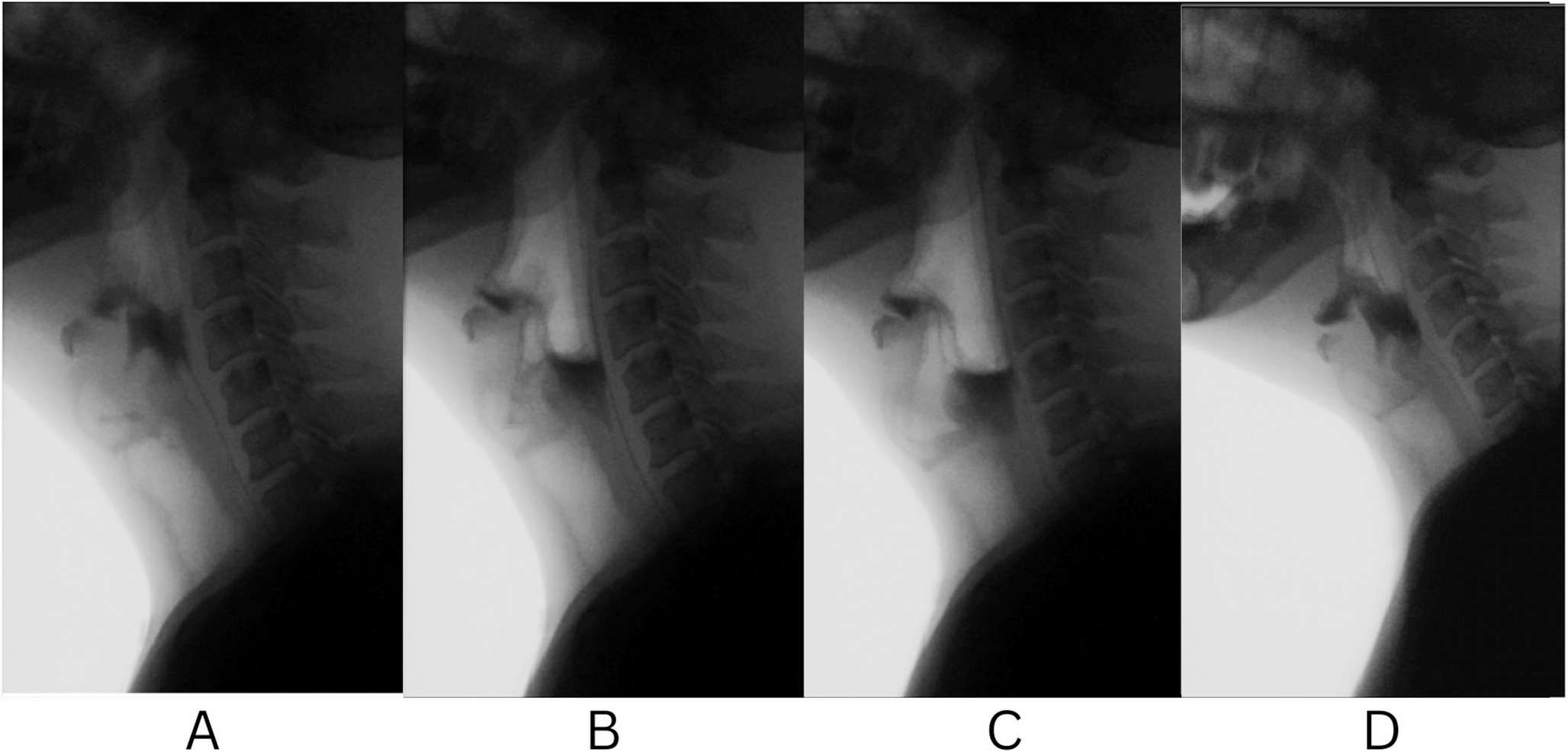
This case is unique because a patient with dysphagia independently acquired vacuum swallowing despite the presence of an open tracheostomy. VF demonstrated that the bolus was rapidly sucked from the pharyngeal cavity into the esophagus. HRM revealed that negative pressure was created in the esophagus during swallowing, accompanied by increased LES pressure, reflecting constriction of the diaphragm. These findings are consistent with previous reports [5, 7,8,9,10].
The most important finding was that a strong negative pressure was generated in the thoracic cavity, even when the lower respiratory tract was open to the atmosphere through the tracheostoma. When inspiratory effort is performed with airway obstruction caused by a closed glottis, a contracted pharynx, and tongue attachment to the palate during vacuum swallowing, a strong negative pressure is created in the thoracic cavity [5, 9, 10]. In this patient, the transient negative intrathoracic pressure during vacuum swallowing was likely generated by a discrepancy between the rapid expansion of the thorax and the delayed expansion of the lungs, reflecting differences in compliance between the chest wall and the lungs. Similar to some previously reported cases, this patient acquired the ability to perform vacuum swallowing spontaneously, without any specific instruction. However, compared to previous reports, this patient exhibited a relatively weaker negative pressure in the esophagus during vacuum swallowing. This may be because the airway was open to the atmosphere through the tracheostomy.
In this case, the swallowing disorder was presumed to be bulbar-type dysphagia caused by a brainstem lesion. The patient exhibited weak pharyngeal constriction and an impaired UES opening, for which laryngeal elevation surgery and cricopharyngeal myotomy were performed. In addition to the surgical interventions, the patient’s self-acquisition of vacuum swallowing may have contributed to the improvement in pharyngeal bolus passage.
Notably, even patients with dysphagia who undergo tracheostomy can achieve vacuum swallowing with appropriate instructions, as reported in previous studies [9, 10]. It is generally considered difficult to generate sufficient negative intrathoracic pressure during swallowing in patients with tracheostomy, because inspiratory effort causes air to flow into the airway, preventing negative intrathoracic pressure generation. However, in this case, effective negative intrathoracic pressure was generated, resulting in vacuum swallowing. This finding is particularly unique even in the presence of an open tracheostomy. Although the patient underwent an open tracheostomy, a stronger negative pressure in the esophagus might have been generated when a valve was used with the tracheal cannula.
At present, vacuum swallowing can only be clearly identified by manometric study. When VF shows very rapid pharyngeal bolus passage, as in this case, performing manometry may reveal this phenomenon. Therefore, some cases may not have been recognized simply because pressure dynamics were not evaluated. Vacuum swallowing may be acquired as a compensatory swallowing method in patients with dysphagia due to weak pharyngeal contraction and impaired UES opening. We believe that vacuum swallowing may also occur in other neurological dysphagia disorders, but it has not been reported to date due to the difficulty of diagnosing it and the fact that many clinicians are not yet aware of this swallowing phenomenon. Further studies are needed to determine whether this phenomenon can also be observed in other similar conditions.
In summary, we report a unique case in which a patient with dysphagia and an open tracheostomy independently acquired vacuum swallowing. Further research is needed to determine whether patients undergoing tracheostomy can consistently acquire vacuum swallowing following instructions.


Comments (0)