
Remember me

Dysphagia is a symptom commonly seen in patients who are undergoing acute inpatient rehabilitation, which may lead to serious complications including aspiration pneumonia. Aspiration of liquids may be due to several factors such as reduced oral containment of the swallow; reduced coordination and timing of the swallow; reduced laryngeal closure; and reduced laryngeal sensation [1]. Previous researchers have shown a relationship between increasing liquid bolus volume and higher risks for aspiration [2,3,4]. While texture modification is a common dysphagia intervention used to promote a safe swallow [1], reducing bolus size is also another common intervention [5].
Previous research has investigated the influence verbal instructions or cues may have upon facilitating a safe swallow. Donzelli and Brady [6] investigated the effects of different types of verbal instruction to attain vocal fold closure to facilitate a safe swallow and reported the most effective verbal instruction was the hard breath-hold group and the least effective was the inhale/easy breath-hold group [6]. Daniels and colleagues [7] investigated the effects of verbal instructions on bolus flow and discovered swallowing function was altered following the use of verbal cues to initiate a swallow. Another study investigated the differences in bolus sizes between natural drinking conditions as compared to instructed experimental cued swallowing conditions and found statistically significant larger bolus sizes with the natural drinking conditions [8].
In clinical practice, a common strategy used to reduce the bolus size to reduce aspiration risk with liquids is to use specific verbal instructions or cues. For example, this may include something as simple as “take a small sip” or providing further cueing to facilitate a small sip such as “take a small sip like its hot coffee”. While these verbal instructions (or similar variations) may be commonly used in clinical practice, it is unknown if there are actual differences in how an individual may respond to specific verbal instructions or cues. The specific objective of this study was to evaluate the effects, if any, different verbal instructions may have on bolus size with self-administration of thin liquids. This project was undertaken as it is important for the dysphagia rehabilitation team to understand the influence, if any, that verbal instructions or verbal cues may have upon bolus size adjustments in clinical practice to facilitate a safe swallow and potentially result in improved patient outcomes.
MethodsParticipantsThis was a prospective, randomized, repeated measure design using two study groups. Group 1, healthy controls, included healthy community volunteers who were 18 or older with no previous history of head/neck cancer, stroke, brain injury, neurologic disease, or swallowing difficulties. The inclusion of healthy adults served two primary purposes. First, it was essential for safety, as all healthy participants completed the study protocol before the investigators proceeded with the patient group. Second, healthy adults were included to establish reference points for the various instructions and delivery methods. Group 2 included acute rehabilitation inpatients following either a stroke or brain injury, who could safely consume thin liquids (dysphagia was not an exclusion criteria). All participants, regardless of study group, were required to have adequate hearing and cognitive skills to follow one-step commands and the physical ability to self-administer a bolus from a cup and straw. Both study groups represented a convenience sample. All study participants in Group 1 completed the study protocol before recruitment began with Group 2. This study was approved by this organization’s institutional review board. All participants signed written informed consent.
ProcedureParticipants in Group 1 and 2 were randomized into either the cup or straw delivery method condition, with participants in the cup condition consuming all eight bolus presentations via open cup, and the straw condition consumed all eight bolus presentations via straw. Each subject consumed eight boluses of room temperature water under the following four verbal instructions: 1. Take a drink; 2. Take a comfortable sip; 3. Take a small sip; 4). Take a small sip like it is hot coffee. The order of instructions was randomized for each subject using a random integer set generator software and each subject had eight cups prepared. Four cups were prepared with 60-mL of water in a 120-mL (4 oz) cup and four cups were prepared with 120-mL of water in a 240-mL (8 oz) cup. The ratio of liquid to cup size was the same between the two cup sizes. The cup and its contents were weighed before and after each administration to extrapolate the volume consumed under each condition. Participants consumed the room temperature water (self-administered) from each cup following the verbal instruction provided by the investigator. The participant received a new cup for each condition/instruction. Each participant consumed a total of eight boluses (i.e., four verbal instructions across two different cup sizes). The timing of when the participants completed the study protocol was not controlled and was based upon schedule availability. Additionally, hydration status and dietary habits were not collected on the participants.
Study Hypotheses/Data AnalysesDescriptive statistics, along with independent t-tests and chi-square analyses, were conducted on the participants’ demographics to characterize the study sample and compare the two study groups. Initially, the entire study sample was analyzed overall by instruction level to assess the mean bolus size consumed, irrespective of study group, vessel size, or delivery method. Additionally, pairwise comparisons of the various combinations of verbal instructions were performed for the entire sample.
The primary objective of this study was to evaluate the effects of different verbal instructions on bolus size during the self-administration of thin liquids. To achieve this, a repeated measures general linear model ANOVA was conducted, comparing the effects of four verbal instructions across two vessel sizes under eight repeated measures conditions, which served as within-subject variables. The model also accounted for between-subject factors, including study sample groups (healthy controls vs. patients) and delivery method conditions (cup vs. straw). The main effects of instruction, patient grouping, vessel size, and delivery method were thoroughly examined. A follow-up independent t-test was completed to compare the mean bolus sizes consumed for vessel size (4-oz vs. 8-oz) regardless of type of verbal instruction, delivery method (cup vs. straw), or study group. All analyses were performed using SPSS version 23.0, with a significance level set at 0.05. To control for Type I error (i.e., the incorrect rejection of a true null hypothesis), a Bonferroni correction was applied post hoc.
ResultsParticipantsOne hundred participants completed the study protocol with an age range from 24–95 years, mean age 54.9 years (SD ± 20.9), 34% male/66% female, and mean height of 66.8 inches (SD ± 3.6). Table 1 summarizes the subject demographics by study group along with the randomization assignments for the cup or straw delivery method condition. Differences between the two study groups for age (t = −14.934, p ≥ 0.0001) and gender (χ2 = 4.456, p = 0.035) were statistically significant with the healthy control group being younger and having fewer male participants. Differences in height between the two groups were not significant (t = −0.288, p = 0.774). Group 2 (patient group) included 28 patients with a stroke and 22 patients following a brain injury. Each participant consumed 8 boluses with a total of 800 boluses available for analysis across all 100 participants. No participants withdrew from the study and all participants were able to complete the study protocol.
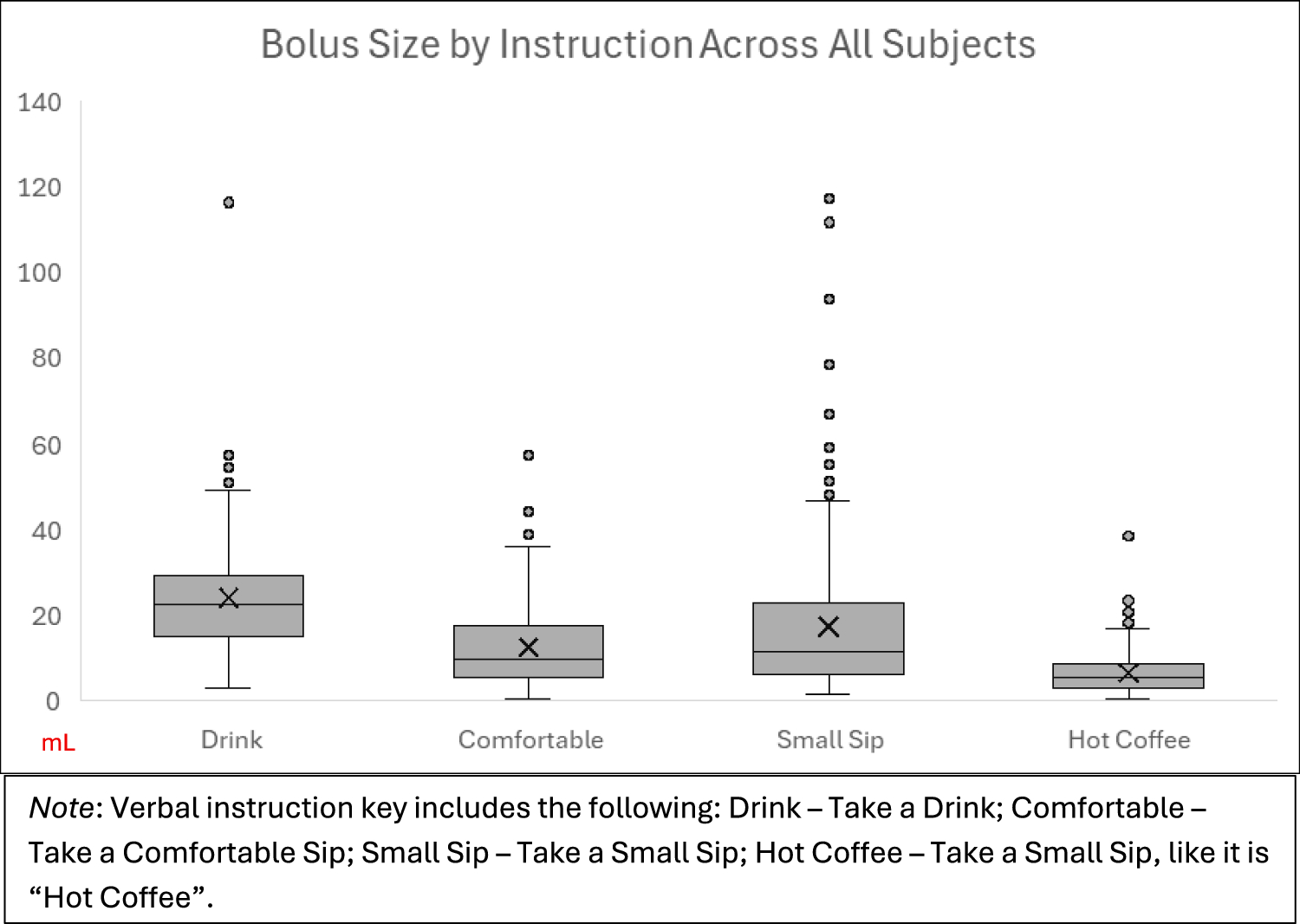
Table 1 Participants demographicsBolus (Sip) SizesTable 2 summarizes the mean amounts consumed across all bolus trials for each verbal instruction, regardless of study group, vessel size, or delivery method, for the entire study sample. Analysis of the overall sample revealed statistically significant differences among the various verbal instructions, with the largest mean bolus size consumed following the instruction "take a drink," and the smallest mean bolus size consumed following the instruction "take a small sip like it is hot coffee." Table 3 presents the multiple comparisons of mean differences in consumption for the entire study sample across the different verbal instructions. With the exception of instruction 3 ("take a small sip") and instruction 4 ("take a small sip like it is hot coffee"), the pairwise comparison differences were statistically significant. Figure 1 offers a visual summary of bolus size by instruction for the entire study sample, displaying the median, quartiles, and potential outliers. Notably, the verbal cue "take a small sip" was associated with the highest number of outliers.
Table 2 Overall Results by Instruction LevelTable 3 Pairwise comparisons of mean differences between verbal instruction for entire study sampleFig. 1
Bolus size by instruction
Table 4 summarizes the main effects of different verbal instructions on bolus size consumed across study groups, vessel size (4-oz vs. 8-oz), and delivery method (straw vs. cup). In this repeated measure analysis, the model included eight factors representing the four verbal instructions across the 4-oz and 8-oz cups (i.e., the 8 boluses provided to each participant). Since Mauchly’s sphericity test indicated a significant violation of sphericity in the model (p ≤ 0.0001), the Greenhouse–Geisser corrected values for the degrees of freedom was employed to adjust for this violation. The within-subject effect revealed statistically significant differences in mean bolus sizes among the four verbal instructions across the two vessel sizes (F = 124.612, df = 2.304, p ≤ 0.0001). The highest mean amount consumed was associated with the instruction “take a drink”, while the lowest mean amount was linked to the instruction “take a small sip, like it is hot coffee”. In contrast, the between subject effects showed that the difference in mean bolus size consumed between the study groups (healthy control vs. patients) was not statistically significant (F = 2.231, df = 1, p = 0.139), indicating that similar amounts were consumed regardless of the study group. Furthermore, the analysis of between-subject effects for delivery method (cup vs. straw) also revealed no statistically significant differences in mean bolus volume consumed (F = 2.097, df = 1, p = 0.151). This finding suggests that the delivery method did not influence the mean bolus size consumed. The follow-up independent t-test conducted to compare the mean bolus sizes consumed, irrespective of verbal instruction, delivery method, or study group, revealed statistically significant differences (t = −3.310, df = 712.54, p ≤ 0.0001). The trials utilizing the smaller vessel size (i.e., 4-oz cup) had a lower mean bolus amount (mean = 13.46 mL, SD = ± 11.12) compared to the trials with the 8-oz cup, which had a mean of 16.69 mL (SD = ± 15.97). This finding suggests that using a smaller vessel size may facilitate the consumption of a smaller bolus during thin liquid trials.
Table 4 Mean Bolus Size by Study Group, Delivery Method, Vessel Size and Verbal Instruction
Comments (0)