Study design and participants
This study was a cluster randomized controlled trial (RCT) conducted from September 2023 to February 2024 across primary schools in Dongguan, China. This trial was prospectively registered at the ClinicalTrials.gov Protocol Registration and Results System (NCT06048406). A detailed research protocol is available in Additional file 1: Trial protocol [5,6,7, 10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28], which was reported elsewhere [29]. The study was approved by the Ethics Committee of the School of Public Health, Sun Yat-sen University (approval number: No. 2023107).
All eligible fourth- and fifth-grade students aged 7–12 years in these schools were invited to participate. Students with contraindications to influenza vaccination, who have received an influenza vaccination within 6 months prior to the study start, diagnosed with influenza or confirmed as influenza-like cases at the commencement of the study, or unwilling to participate in the project, were excluded. All students and their parents or guardians gave written informed consent before participation.
Randomization and blinding
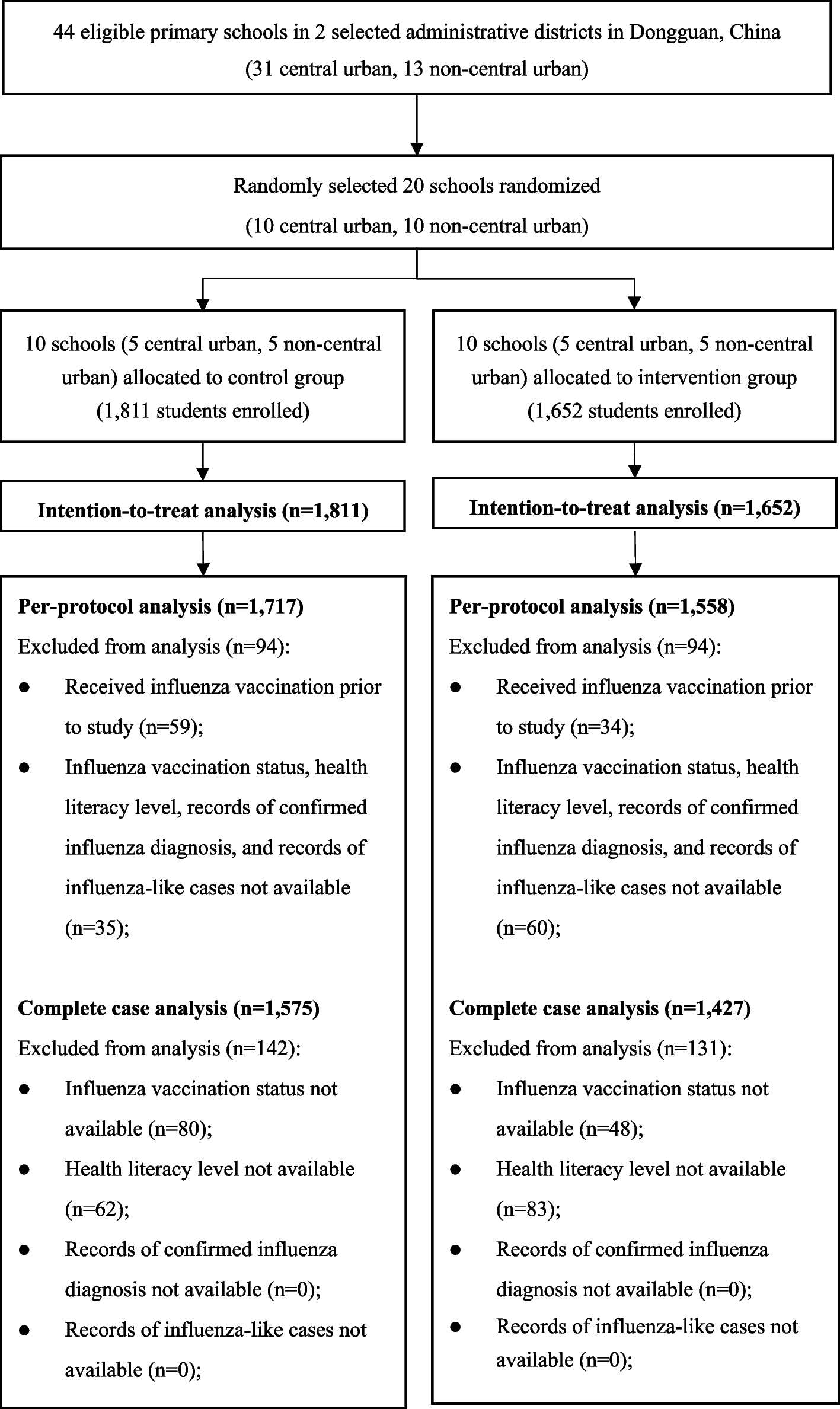
This study used stratified randomization based on two administrative districts in Dongguan, one in the central urban area and the other in the non-central urban area. Within each district, ten primary schools were randomly selected. Schools were then randomly assigned in a 1:1 ratio to either the intervention or control group. The allocation sequence was generated through simple random sampling by a computer program, managed by an independent assistant who was blinded to schools. Given the nature of the intervention, it was not possible to blind participants or the personnel delivering the intervention. However, to preserve the integrity of the study outcomes, both the outcome assessors and the data analysis were blinded to the group allocation, ensuring unbiased evaluation of the effectiveness.
Intervention
Participants in the intervention group received a multifaceted health education package designed to enhance influenza vaccination literacy. In contrast, the control group continued with the standard health education provided by the schools, without additional components. The intervention period was from September 2023 to February 2024, during which the intervention group received targeted health education interventions monthly.
The intervention package included educational activities, distribution of educational booklets, four consecutive monthly reminders of vaccination, and distribution of vaccination souvenirs. Educational activities consisted of four monthly 40-min classroom lectures (September 2023–January 2024) covering influenza transmission, vaccination importance, vaccine mechanisms, and preventive health practices. Lectures were delivered by medical professionals and public health experts with experience in child education. Sessions were interactive, incorporating visual aids, structured activities, and Q&A sessions. Educational booklets, developed in collaboration with the Center for Disease Control and Prevention of Dongguan City (Dongguan CDC), were distributed to reinforce key messages. Parents received four consecutive monthly reminders from teachers about vaccination. Additionally, the intervention included the distribution of “Epidemic Prevention Little Guards” medals as vaccination souvenirs to incentivize participation. Souvenirs were distributed to schools prior to the intervention, and all vaccinated students in the intervention group received them from their teachers.
Data collection
Data were collected at two time points: at baseline in September 2023 and at the conclusion of the intervention in February 2024. Both students and parents or guardians participated in the study by completing self-administered questionnaires designed to capture a comprehensive range of information. The questionnaires assessed socio-demographic characteristics, personal health history, and levels of health literacy related to influenza vaccination. Follow-up data collection in February 2024 encompassed the updated health literacy assessments, vaccination status, influenza cases, and the influenza-like illness (ILI) cases.
Influenza cases were identified using records from the municipal CDC influenza surveillance network. Furthermore, the ILI was defined as instances of fever (body temperature ≥ 38 °C) with a cough or sore throat, with epidemiological evidence or a positive influenza rapid antigen test, and excluding other causes of similar symptoms. Identification of ILI cases was conducted through a school-based case reporting system, in which trained school medical staff and teachers monitored and recorded symptoms. This system, launched by the Department of Education of Guangdong Province, facilitated standardized illness reporting across participating schools. It also included a morning inspection and absenteeism registration system, where teachers monitored unexplained absences and contacted parents to determine if symptoms aligned with ILI criteria.
Outcomes
The primary outcome was the influenza vaccination rate of students, which was determined by records from the CDC vaccination system. Secondary outcomes included the influenza vaccination health literacy levels, influenza incidence, the ILI incidence, and the influenza vaccine protection rate.
Influenza vaccination health literacy was assessed across four dimensions: knowledge, attitude, behavior, and skills. To account for differences in knowledge and understanding between children and parents, the children’s questionnaire contained 12 questions (knowledge: 7, attitude: 2, behavior: 2, and skills: 1), whereas the parental version contained 33 questions (knowledge: 9, attitude: 15, behavior: 6, and skills: 3). In the children’s questionnaire, knowledge, attitudes, and behaviors were single-choice, with correct responses scoring 1 point and incorrect answers scoring 0. The skills question was multiple-choice, with each correct option receiving 1 point (total of 6 options). The total score ranged from 1 to 17. In parental questionnaire, knowledge questions were single-choice, scored similarly to the children’s version. Attitude questions used a five-point Likert scale (0 to 4 points) to capture varying levels of health literacy. Behavior questions consisted of two binary-choice items (scored 0 or 1) and four three-option items (scored 0–2). Skills questions included two single-choice questions (scored 0 or 1) and one multiple-choice question (total of 6 points). The total parental health literacy score ranged from 1 to 87, distributed as follows: 0–9 for knowledge, 0–60 for attitudes, 0–10 for behavior, and 0–8 for skills.
The influenza incidence was calculated as the number of individuals diagnosed with influenza divided by the total number of individuals, multiplied by 100%. The ILI incidence was calculated as the number of ILI cases divided by the total number of participants, multiplied by 100%. The influenza vaccine protection rate was calculated as the difference between the incidence rate in unvaccinated individuals and the incidence rate in vaccinated individuals, divided by the incidence rate in unvaccinated individuals, multiplied by 100%.
Sample size
Based on the assumption that the anticipated influenza vaccination rate is 80% in the intervention group and 50% in the control group, the power of 0.8, and the two-sided α level of 0.05, approximately 1380 primary school students were required in each group [26, 27]. To account for potential sample attrition, the sample size was expanded by 10%, resulting in a final estimated total sample size of 3036 for statistical analysis.
Statistical analysis
Data were analyzed according to intention-to-treat (ITT) analysis and per-protocol (PP) principles. The ITT analysis included all participants as originally randomized, regardless of adherence, ensuring the benefits of randomization were preserved and providing a pragmatic estimate of the real-world effectiveness. The PP analysis focused on participants who adhered to the study protocol, offering insights into the intervention efficacy under ideal adherence. Continuous variables were described using means ± standard deviation (SD) or median (interquartile range), depending on their distribution. Group comparisons were performed using two independent samples t-tests or Wilcoxon rank-sum tests. Categorical variables were reported as frequency and proportions, with comparisons made using chi-square tests or Fisher’s exact test as appropriate. The effectiveness of the intervention on the influenza vaccination rate, health literacy levels, and the incidence of influenza and ILI was assessed using log-binomial regression, linear regression models, and Poisson regression, respectively. Given the possible residual imbalance in baseline characteristics after cluster randomization, we adjusted for town, sex, grade, father’s age, mother’s age, father’s education, mother’s education, father’s occupation, mother’s occupation, family income, number of siblings, and parent-rated child heath in the models. These models provided estimates of adjusted risk ratios (RRs), adjusted regression coefficients (β), and adjusted incidence rate ratios (IRRs), along with 95% confidence intervals (CIs). Exploratory subgroup analysis was conducted to explore potential differences in effect sizes by town, grade, and sex, using P values for interaction to examine heterogeneity across subgroups.
To address the potential impact of missing data, prespecified sensitivity analyses were conducted by repeating the analyses after excluding children with missing data for either outcome variable (n = 273). By combining ITT analysis, PP, and sensitivity analyses, we aimed to maintain the rigor of our statistical evaluation while addressing limitations related to missing data. All analyses were performed using Stata/MP version 18 (Stata Corp).


Comments (0)