Our aim was to follow-up initially SARS-CoV-2-infected (PCR +) and SARS-CoV-2-naïve (PCR −) adults residing in South-Eastern Norway with questionnaires and evaluate levels of antibodies against the SARS-CoV-2 S and N proteins at 12 and 24 months after their initial PCR tests in 2020. We then assessed the persistence and possible predictors of high antibody levels against S protein.
Study design and data sources
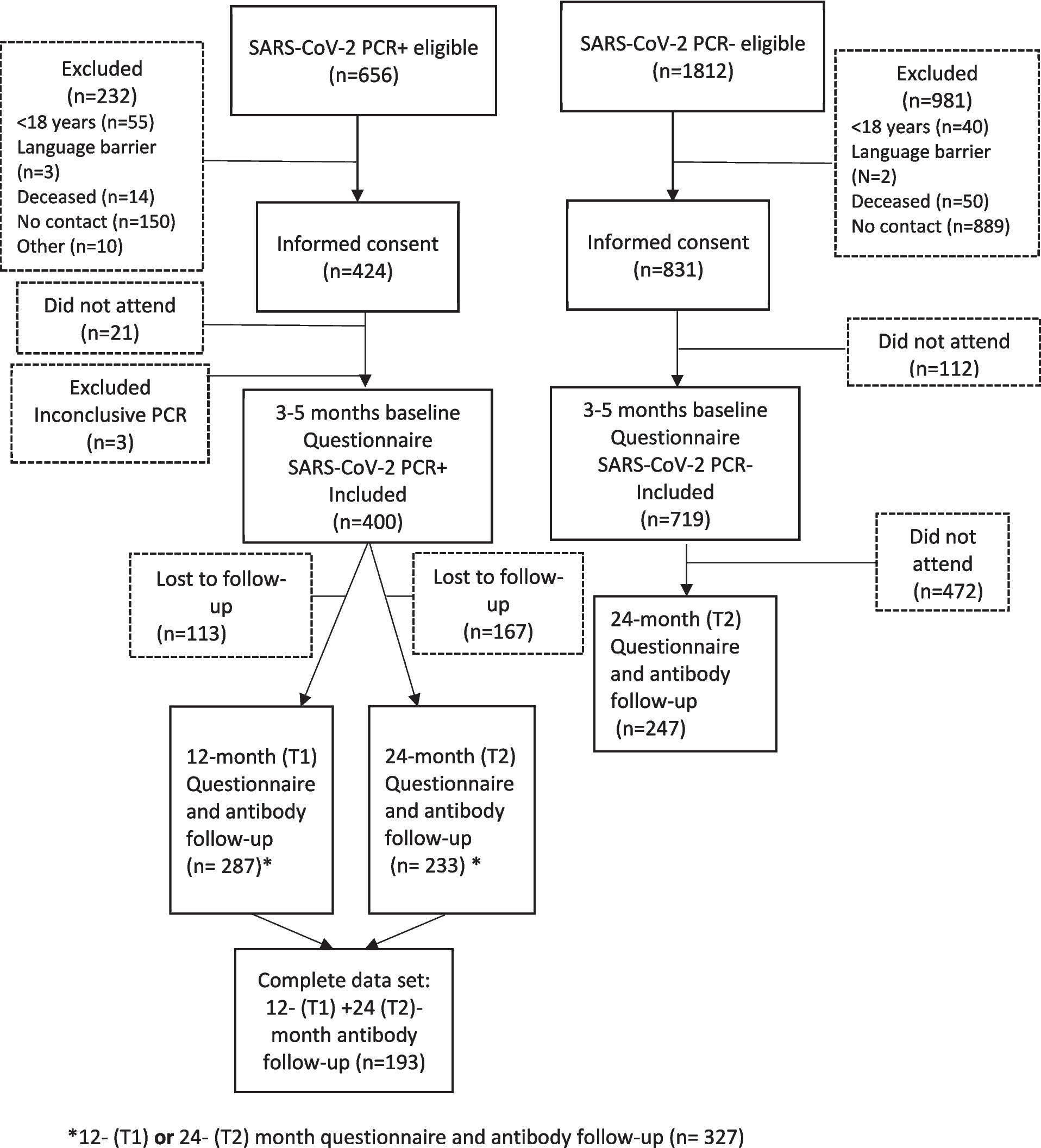
This multicenter cohort study included individuals from all hospitals, municipal laboratories, and test centers in the region. The cohort was chosen from PCR + and PCR − adults (≥ 18 years of age) living in South-Eastern Norway (Agder and Telemark counties) who were reachable by phone during the inclusion period (between February 28 and December 17, 2020—between the first and second waves of the pandemic). Participants who could not answer the questionnaire in Norwegian were excluded.
We included baseline data (defined as the time of the first questionnaire) for the PCR + participants, 3–5 months after the first PCR test, and from a shorter follow-up questionnaire at 12 months (interquartile range [IQR]: 9–12 months), defined as T1, as well as at 24 months (IQR: 23–26 months), defined as T2. T1 ranged between January 21, 2021 and February 9, 2022, and T2 between March 23, 2022 and January 10, 2023. Antibody and questionnaire follow-up data for the PCR − participants was available at T2. The median antibody levels against S protein at T1 and T2 were also stratified by age groups for the PCR + participants with paired measurements (n = 193/400). We have previously reported on natural immunity in this cohort between 2020 and 2021, as well as risk factors for SARS-CoV-2 infection [5, 21].
Study population
The criteria for SARS-CoV-2 testing changed in Norway over the study period but there were no differences between the PCR + and PCR − participants. In the first wave of the pandemic in Norway, the symptomatic patients were tested using PCR. In the second wave, also close contacts and asymptomatic individuals were tested during the outbreaks [22]. We used the results of the first PCR test for each participant. We aimed to include all of the eligible PCR + and PCR − participants in a 1:2 ratio, matched according to the time of PCR testing and geographical location during the study period.
Laboratory methods
Antibodies against the SARS-CoV-2 S and N proteins were tested in serum samples collected from the PCR + participants at 12 and 24 months following their initial PCR tests and at 24 months following their initial PCR tests for the PCR − ones.
The serum samples were prepared from whole blood centrifuged for 10 min at 3000 rpm and stored at − 80 °C for further analysis. All antibody analyses were performed using a Cobas 801 fully automated system (Roche Diagnostics, Mannheim, Germany). An Elecsys Anti-SARS-CoV-2 S electrochemiluminescence immunoassay (Roche) was used to quantitatively measure antibody levels against the S protein. This immunoassay quantifies total antibodies using a recombinant protein that represents the receptor-binding domain of the S protein in a double-antigen sandwich assay format. All tests and analyses were performed according to the manufacturers’ instructions. The cutoff value for units per milliliter (U/mL) was > 0.8 U/mL. Owing to the exceptionally high concentrations of antibodies against the S protein at 24 months, samples of > 250 U/mL were diluted several times and re-measured. Dilutions of 1:10, 1:50, and 1:400 yielded a measuring range of 0.4–100,000 U/mL. The Elecsys Anti-SARS-CoV-2 electrochemiluminescence immunoassay was used to detect antibodies against the N protein. A double-antigen sandwich assay was used to assess antibodies against the S protein, with the recombinant protein being represented by the N protein. Antibodies against the N protein were analyzed and interpreted according to the manufacturer’s instructions, with a cutoff index of > 1 being considered positive.
Vaccination status
A unique personal identification number linked each participant to the Norwegian Immunization Registry (SYSVAK), providing information regarding the type and date of COVID-19 vaccine doses received between January 2021 and January 2023. The SYSVAK represents a national electronic registry that records every vaccine received by individuals in Norway [23].
Data collectionQuestionnaires
We used questions from the Norwegian Institute of Public Health’s COVID-19 questionnaire, the Telemark study’s questionnaire [24, 25], as well as several questions that were unique to this study. Sociodemographic data, such as age, sex, education, and income, and lifestyle factors, such as body mass index (BMI), smoking status, symptoms at baseline, and pre-existing comorbidities, were obtained from a self-reported questionnaire. Symptom and comorbidity scores were calculated by adding the number of symptoms from 0 to 13 (coughing, running or stuffy nose, sore throat, pain upon swallowing, dyspnea, headache, fever, fever with chills or sweating, pain in the stomach, nausea or diarrhea, impaired sense of smell or taste, myalgia, and dizziness) or comorbidities from 0 to 9 (asthma, chronic obstructive pulmonary disease, other lung diseases, cancer, heart disease, hypertension, diabetes, musculoskeletal disease, or any other disease) for each participant. Each symptom and comorbidity was considered equally. All positive PCR tests and commercially available SARS-CoV-2 antigen tests reported by the participants during the follow-up period were recorded. COVID-19 vaccination status was reported based on the date and type of vaccine received.
Statistical analysis
We did not conduct statistical power calculations because it was unclear in advance how many participants would be eligible for inclusion over the study period. The normality of the distribution of all continuous variables was assessed using the Shapiro–Wilk test. Medians and IQRs were used to express non-normally distributed variables. Wilcoxon rank-sum and Kruskal–Wallis tests were used to compare differences in median dispersions between groups, as appropriate. Dunn’s test was applied with Bonferroni correction for multiple comparisons. Categorical variables were expressed as frequencies and percentages and compared using Pearson’s chi-squared or Fisher’s exact tests, as appropriate.
Antibody levels against the S protein at 24 months were categorized as high or low, based on the 50th percentile. The cutoff value for antibodies against the S protein was 9890 U/mL. Possible predictors of high antibody levels against the S protein at 24 months were studied using both univariate and multivariate logistic regression models. Regression analysis results were calculated and presented as odds ratios (ORs) with associated 95% confidence intervals (CIs). All statistical analyses were performed using STATA version 18.0 (StataCorp, College Station, TX, USA). Statistical significance was set at p < 0.05.
Our returned questionnaires had missing data, ranging between 0.4 and 7.3% for certain questions. All variables with missing data were assessed and found to be random, so imputation was not performed for the missing data.
Ethics
Participation in the study was voluntary. After verbally agreeing to participate at the time of the baseline survey, all of the participants also provided written informed consent prior to being included. The participants then completed the first questionnaire on paper. Shorter online follow-up questionnaires were then completed at T1 and T2 for the PCR + participants and at T2 for PCR − ones. The PCR − participants initially only consented to participate at the time of the baseline survey; however, following a revised written agreement, they were later recruited for the 24-month follow-up survey as well. The study was approved by the Regional Committee for Medical and Health Research Ethics of South-East Norway (ID: 146,469).
Patient and public involvement
Two user representatives were involved, according to the Norwegian National Guidelines for User Involvement in Health Research (May 2018). They played an important role in all phases of the project—particularly regarding the development and testing of the questionnaires. They helped us to better understand the patients’ points of view and provided valuable feedback concerning our study protocol, methods, information, consent forms, questionnaires, and dissemination of the results.


Comments (0)