Principal findings
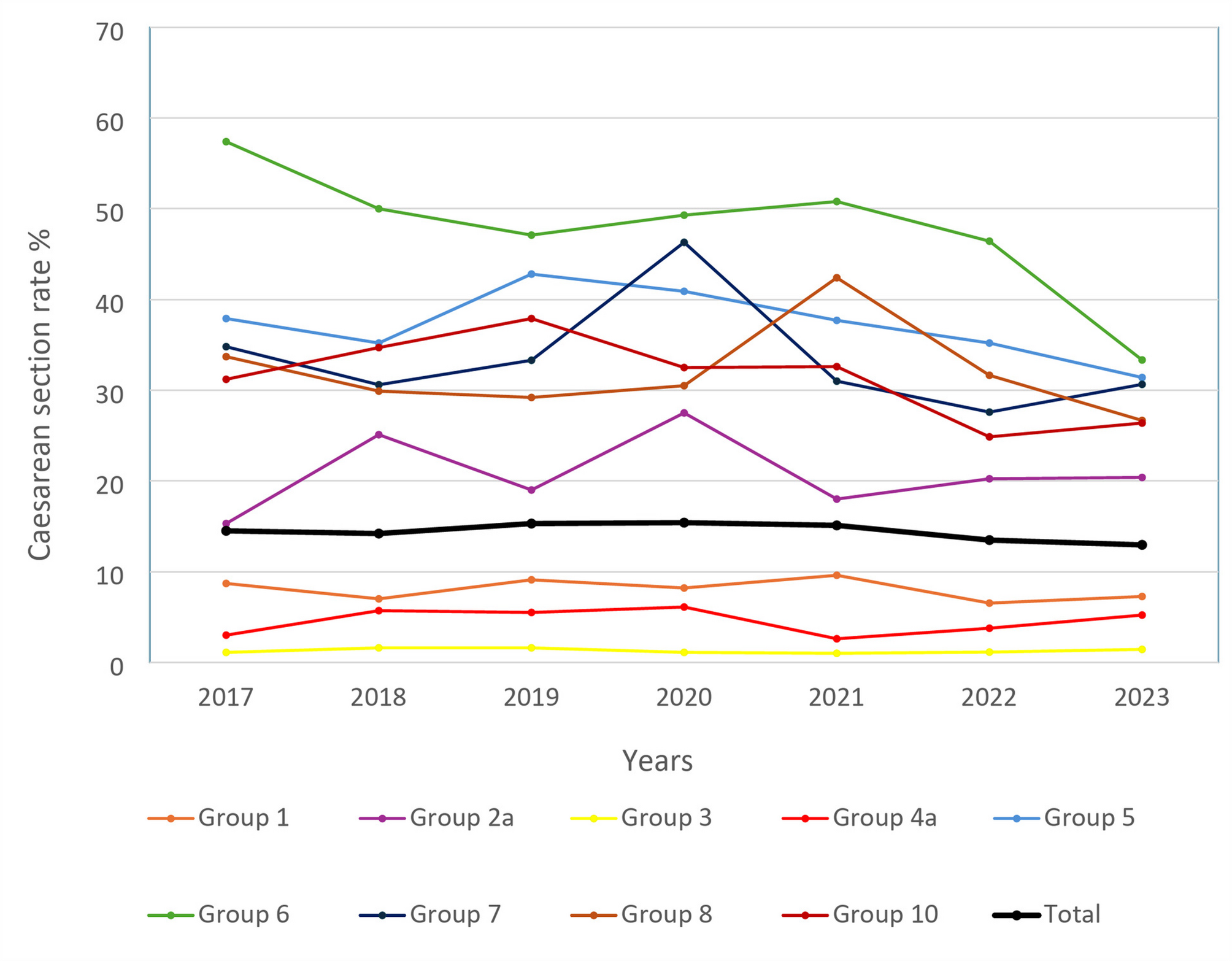
The Robson classification was used to evaluate trends in CS rates within a level III university maternity hospital in Besançon, France. An average CS of 15% was maintained over 7 years with stable maternal and neonatal outcomes. Importantly, a significant downward trend in CS rates, reaching 13% in 2023, was observed. By opposition to international data and future forecasts [12] predicting a constant increase in CS rates, our data shows that it is possible to control the CS rates and even to reduce them in a French level III maternity. Our analysis highlighted that this reduction was mostly driven by a significant reduction of CS among group 5 and group 6. Additionally, it is likely that the change in obstetrical practices is associated with an increase in inductions rates.
Results
Our data highlights potential strategies to control the constant rise in CS rates worldwide. Among them is reducing the number of repeated CS among women with a previous CS. Similarly to what is reported worldwide, group 5 was the largest contributor to the relative and absolute CS rates. Nevertheless, the stability of the size of group 5 over the study period underlines the importance given in our unit to promote vaginal deliveries for patients with a previous CS and reducing the number of patients with multi-scarred uterus, for whom the management of childbirth is much more difficult and riskier. As such, the absolute contribution to the overall CS rates was lower (3.2%) than what has been reported in other high income countries (4 to 10.0%) [13, 14]. In our institution, all patients with a scarred uterus are seen by an obstetrician to discuss the mode of delivery, which is subsequently validated in our multidisciplinary obstetrical staff. No ultrasound criteria, particularly the measurement of the thickness of the lower segment, are used to select candidates for a trial of labor after cesarean (TOLAC), as suggested by others [15]. Furthermore, a single previous CS is not a contraindication to induction in our center, for which balloon ripening, artificial rupture of the membranes or oxytocin may be used. Like other patients, they can benefit from a two-day cervical ripening phase using a balloon, before using oxytocin. There is no contraindication to attempt a vaginal delivery even if fetal macrosomia is suspected, and they can continue beyond the term of pregnancy to maximize spontaneous onset of labor. Oxytocin can be used to for labor augmentation with adequate monitoring of the contractions; if needed an internal tocometry is used. Patients with double-scarred uteri are allowed to attempt a vaginal delivery but only if labor begins spontaneously. We strive to give these patients the best possible chance of a natural birth, and the management of the various stages of labor is similar to that of other patients except oxytocin for labor augmentation is not used. Oral consent is obtained, and patients are warned of the higher risk of emergency CS and uterine rupture during TOLAC. A major fear of TOLAC is the risk of uterine rupture. Interestingly, despite having a higher rate of vaginal birth after CS, the number of uterine ruptures was low (i.e. 3–4 cases per year) and comparable to what is reported in literature [16]. During the study period, uterine ruptures were clearly predominantly represented in group 5. Given the very low number of events, no conclusions can be drawn, but neither the use of oxytocin nor the induction of labor appeared to be a determining factor in the occurrence of the rupture in this group. Our findings further strengthen the importance of providing adequate care to women with a previous CS as these represent the main driver of the overall CS rate. Recent European data [14], indeed, demonstrated similar findings, with countries achieving CS rates below 30%, having an absolute contribution to the CS rate of group 5 < 10%, compared to countries with a higher rate of CS for which the contribution of group 5 could reach 10 to 18%.
Another important target is the management of non-cephalic presentations. We observed a significant reduction in the CS rate of group 6 over the study period, which may have contributed to the reduction in the overall CS rate observed. Our institution does have a strong policy of promoting vaginal breech delivery. During the study period, vaginal breech deliveries were achieved in 52% and 63% among primiparous and multiparous, respectively. The Hannah study [17] demonstrated an increased perinatal morbi-mortality in the case of vaginal breech delivery, leading to the abandonment of this practice in many centers worldwide. Since then, other studies have demonstrated, that among selected candidates there was no increased risk of immediate adverse neonatal outcomes in the case of planned vaginal deliveries [18]. Similarly, we did not observe an increased risk of adverse outcomes despite a 24% reduction of CS rate among group 6. In our unit, selection of candidates is based on the French national recommendations and the protocol has been previously published [19, 20]. Precisely, all cases are discussed within our obstetrical multidisciplinary meeting. Primiparous benefit from a pelvimetry CT-scan, while twins and multiparous women with a previous uncomplicated vaginal birth are allowed a trial of labor without a prior pelvimetry. Induction may be offered in case of a favorable cervix. Additionally, since 2019, we have established a city-hospital obstetric staff, allowing independent professionals (midwives and doctors) to be involved in the discussion regarding the mode of delivery, which may facilitate adherence.
Thirdly, although the design of this study does not allow us to draw any definite relation between the induction and the CS rates, we did observe a significant increase in the induction rate, going from 16.7% in 2017 to 22.7% in 2023. The ARRIVE trial suggested a positive benefit of induction among low-risk nulliparous women on CS rates [21] an effect that was further confirmed in a larger observational study [22]. Our data regarding induction rates follow the national and international trends following the publication of the ARRIVE trial. This increase is mainly linked to a re-evaluation of our induction protocols, particularly for fetal growth disorders (IUGR and macrosomia), in line with international recommendations encouraging induction at 39 weeks of gestation. Moreover, the increased proportion of women with a BMI > 25 kg.m2 women > 35 years old and nulliparous women from 2017 to 2023 contribute to increase our induction rate for maternal indications. Therefore, we may suspect that this contributed to the overall reduction in the CS rates observed.
Clinical implications
Collegial decisions among staff and the daily morning review of obstetrical records allow the team to constantly consider the need for CS so as not to trivialize it. As, the CS-rate in group 1 remained stable during the period, and the size of group 5 did not increase, we are now benefiting from the results of a policy favorable to vaginal delivery for several years, which creates a virtuous circle. We also have very few requests for CS on maternal request. While CS on maternal request would be considered, these situations are discussed as early as possible in collaboration with the private practitioner in charge of the pregnancy, during weekly community-hospital staff meetings. The prevalence of adverse maternal outcomes was lower than described in the French perinatal survey [8]. The prevalence of an umbilical cord arterial pH < 7, which defined pathological fetal acidaemia [23] in our study ranged between 1.3% and 1.8%, and the proportion of newborn with an APGAR < 7 at 5 min of life was stable during the period with an average rate over the 7 years of 1.2%. This proportion is slightly lower than what was reported in the 2021 French perinatal survey and recent Swedish data [8, 24]. Although pH values have a low predictive value for neonatal morbidity [25, 26], they remain commonly used to guide neonatal care and are often used in case of a legal issue. Therefore, this parameter is frequently used to assess obstetrical practice. The diagnostic criteria for neonatal hypoxic-ischemic encephalopathy are more complex and depend on pathologic acidemia, low APGAR score, presence of multiple organ-system failures, and clinical evidence of encephalopathy [27]. The rate of NICU transfer, which may reflect more on the neonatal well-being, was low during the study period. 2.2%, in comparison to what has been reported in other studies [28,29,30].
One of the main concerns of CS is respiratory distress of the newborn, which is 2 to 3 times higher compared to vaginal births [31]. Interestingly, we observed a higher rate of neonatal transfer the same year as our highest rate of CS. While we cannot exclude that more newborns were transferred in the context of the SARS-CoV-2 pandemic, an increased prevalence of respiratory distress may have played a role. No difference in NICU admission rates was observed in our study. Nevertheless, due to the retrospective nature of the study and the rarity of the outcome, we cannot exclude that the study was not powered enough to detect a significant difference. Interestingly, a large Norwegian cohort study recently showed a reduction of fetal intrapartum, perinatal, and neonatal mortality rates associated with a reduction of CS rates from 2008 to 2018, with CS rates similar to ours [32]. A recent large meta-analysis published in 2023 compared maternal and neonatal outcomes in case of planned CS versus a trial of labor. In this review, a planned CS was associated with a reduction of low umbilical artery pH, birth trauma, hypotonia, and chorioamnionitis. Nevertheless, similarly to our results APGAR score and NICU admissions were similar in the two groups. In term of maternal outcomes, urinary incontinence and painful perineum was more frequent in the trial of labor group. Wound infections were more frequent in case of a planned CS; global pain score was not assessed. This meta-analysis reinforces the importance of providing a comprehensive review of the risk and benefit of one birth method versus another to allow an informed choice [33]. Similarly, CS is known to be associated with increased blood loss for the mother [34]. Recent studies on PPH reported an increasing incidence over the last decades, particularly in high-income countries, with a doubling rate reported in several countries, reaching 2–10% [35, 36]. Although multifactorial, the impact of increasing CS rates is questionable. In our study, groups with a higher rate of CS presented a higher risk of PPH. Similar findings were observed among the Swedish population, with the highest absolute rates of PPH observed in group 4b and the lowest in group 3 [36].
Finally, questions remain about the optimal mode of delivery in case of preterm delivery. The Robson classification was originally designed for term pregnancies and may not fully capture the complexity and clinical nuances of preterm labor and delivery. Preterm births often have different clinical indications for cesarean section, such as fetal distress or maternal complications, which may not be fully differentiated within the Robson 10 group (All cephalic births under 37 weeks of gestation). When analyzing preterm births with the Robson classification, it is important to supplement with additional clinical data to understand the context of delivery decisions. Thus, researchers and clinicians should be cautious in interpreting cesarean rates in preterm groups, considering the higher clinical complexity. The available body of evidence does not allow specific recommendations about the choice of mode of delivery regardless of fetal presentation [37]. This lack of recommendation explains worldwide disparities in CS rates in group 10 [14, 38]. Although the absolute contribution to the overall CS rate was high in our unit (2.2%), underlining the high number of preterm births managed in our center, the CS rate in this group was 31.6% and comparable to what is reported in other countries with low CS rates [14]. Although we did not report long-term evolution, our good immediate neonatal outcomes in this group are encouraging regarding the possibility of vaginal delivery in case of preterm birth.
Research implications
While we cannot conclude on an ideal rate of CS, which may not exist and might depend on the local population and obstetrical practices, our study may help other centers assess their own rates. Additional international systematic studies are needed to better describe CS rates and related maternal and neonatal outcomes. The WHO has launched a platform that should facilitate such analysis [39]. Studies should also focus on assessing long-term outcomes. These are necessary (1) for local quality control and center-dependent improvement of practices and (2) for further understanding factors implicated in CS rates at a global level and optimization of obstetrical practices to improve maternal and neonatal outcomes. The role of induction of labor should be specifically tackled. Although it may be associated with a reduction of CS. Specific candidates who may benefit from induction remain to be better defined. Additionally, the impact on other maternal and neonatal outcomes should be assessed. Particularly, potential association with PPH and maternal experience should be considered.
Strengths and limitations
The major strength of this study is the exhaustive collection of data regarding the Robson classification and the low number of missing data for the different judgment criteria, enabling a comprehensive analysis over a 7-year period. At this time, our results are the only data from a French university maternity hospital to be declared on the WHO platform [39]. Several limitations need to be acknowledged. Firstly, our analysis focused on the Robson classification, which relies on minimal characteristics that are not enough to explain CS rates. As such, information regarding indication for induction of labor, indication for CS delivery, fetal complications (e.g., growth restriction, anatomical anomalies) and maternal comorbidities such as diabetes and preeclampsia were not reported. However, our population is comparable to other level III maternity units in France in terms of maternal age, BMI, parity and birth weight of newborns, allowing comparisons [8]. Secondly, our analysis focused on a limited number of maternal and neonatal outcomes routinely collected in our databases. Rates of neonatal trauma, such as fractures and hematoma were not considered. These are often diagnosed within the first days of life and recorded in the newborns’ charts, making them difficult to assess using routine obstetrical files. Thirdly, our analysis focused on immediate neonatal and maternal outcomes, limiting conclusions. CS rates cannot be taken as an endpoint on their own and interpreted in views of immediate maternal and neonatal outcomes. Mode of delivery may, indeed, have additional long-term impact. Important aspects that need to be considered are psychological consequences, sexual and continence dysfunctions, chronic pains, future pregnancy complications, impact on children’s neurocognitive development and risk for chronic disease development later in childhood [40]. The maternal experience of childbirth is taking on an increasing role in maternity wards. In our study, maternal satisfaction was not assessed. Nevertheless, in recent years, we have not observed a significant increase in requests for cesarean sections for maternal convenience in our population. On the contrary, our patients increasingly wish to return to a birth with the least possible medical intervention. Informed consent and shared decision making plays a major role in maternal satisfaction. Comprehensive analysis as presented in our study, contributes to the body of data and might help to adequately inform women in order for them to make the best decision regarding the mode of delivery. Finally, we know that the generalization of our data raises questions. Although comparable to the national population in our case, the evolution of maternal characteristics such as BMI is not the same everywhere around the world and can account for the CS-rate results. Moreover, the promotion of the attempt of vaginal delivery concerning non-cephalic presentations and twin pregnancies is based on decades of knowledge transmission, and reversing after the gradual abandonment of such practices is difficult.


Comments (0)