
Remember me

Globally, the number of reported incident cases declined from 49,637,961 (95% uncertainty interval (UI): 37,364,984–63,774,614) in 1990 to 42,385,827 (95%UI: 32,538,623–53,751,065) in 2019, representing a 15% reduction (95%UI: 9–19%) (Table 1). The age-standardized incidence rate (ASIR) decreased from 1703.56 (95%UI: 1288.59–2179.36) to 1098.36 (95%UI: 843.01–1391.51) per 100,000 population over three decades, with an estimated annual percentage change (EAPC) of -1.44% (95% CI: -1.49%, -1.40%) (Table 1). The upper limit of the 95% CI was below 0, confirming a significant downward trend in ASIR. A total of 19,565 (95%UI: 16,319–23,373) deaths occurred worldwide in 2019, marking a 67% (95%UI: 61–73%) reduction compared to 59,475 (95%UI: 51,678–68,097) in 1990 (Table S1). The global age-standardized death rate (ASDR) in 2019 was 0.5 (95%UI: 0.41–0.59) per 100,000 population, with an EAPC of -5.21% (95%CI: -5.38%, -5.04%), showing a decreasing trend from 1990 to 2019 (Table S1). In 2019, abortion and miscarriage accounted for 1,130,038 (95%UI: 947,675–1,338,397) DALYs globally, marking a 67% decline (95%UI: 61–73%) since 1990. The age-standardized DALY rate was 28.86 (95%UI: 24.21–34.15) per 100,000 population, with an EAPC of -5.14% (95%UI: -5.31%, -4.96%), indicating a sustained decrease over three decades (Table S2).
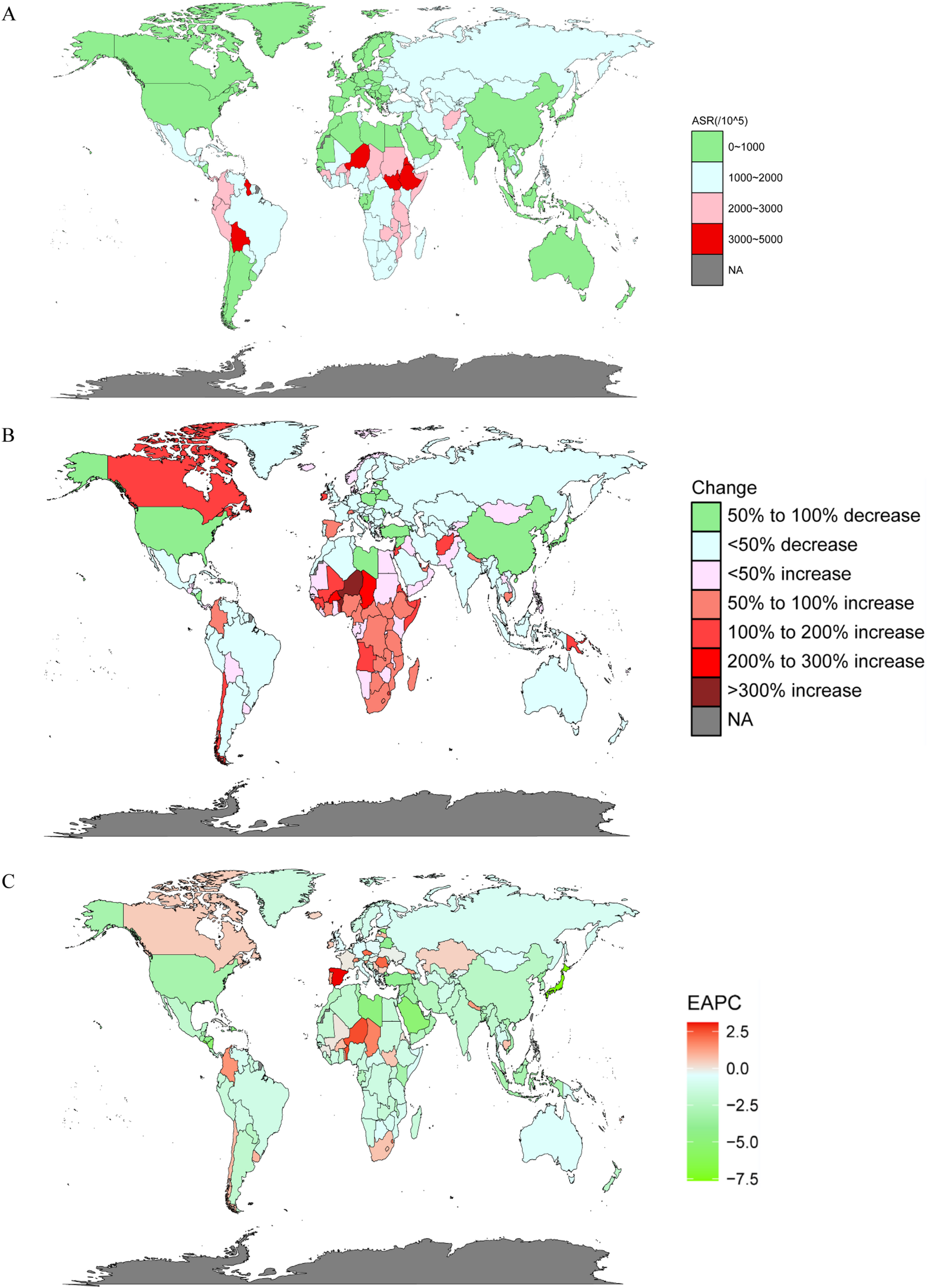
Table 1 The incidence cases and age-standardized rates of maternal abortion and miscarriage in 1990 and 2019, and their temporal changes from 1990 to 2019, for female, in global, SDI regions and 21 GBD regionsIn 2019, the highest ASIR of abortion and miscarriage was in Ethiopia (3839.06 (95%UI: 2900.13–4987.39) per 100,000 population), followed by Bolivia (Plurinational State of) (3524.897 (95%UI: 2622.06–4530.11) per 100,000 population), and Niger (95%UI: 3293.98 (95%UI: 2469.62–4304.95) per 100,000 population) (Fig. 1A; Table S3). Singapore (60.13 (95%UI: 50.48–71.26) per 100,000 population) had the lowest ASIR in 2019, followed by Brunei Darussalam (148.03 (95%UI: 112.05–192.71) per 100,000 population), and Republic of Korea (182.97 (95%UI: 133.21–250.89) per 100,000 population) (Fig. 1A; Table S3). The largest change in incident cases was in Niger (365% (95%UI: 288–433%)) from 1990 to 2019, while the greatest decrease in incident cases was in Japan (-80% (95%UI: -84%, -75%)) (Fig. 1B; Table S3). Moreover, Japan (-7.63% (95%CI: -8.67%, -6.58%)) showed the greatest decrease by the EAPC in ASIR (Fig. 1C; Table S3).
Fig. 1
The incidence of abortion and miscarriage in 204 countries and territories. A The age-standardized incidence rate (ASIR) of abortion and miscarriage in 2019. B The percent change in incidence cases of abortion and miscarriage from 1990 to 2019. C The estimated annual percentage change (EAPC) of abortion and miscarriage in ASIR from 1990 to 2019
In 2019, Chad had the highest ASDR at 17.59 per 100,000 (95%UI: 12.09–23.84), followed by Niger at 14.02 per 100,000 (95%UI: 9.2–19.75) (Figure S1A; Table S4). Chad also showed the largest increase in deaths, rising by 109% (95%UI: 37–201%), while the number of deaths decreased by 100% (95%UI: 99–100%) in Bosnia and Herzegovina from 1990 to 2019 (Figure S1B; Table S4). The greatest reduction in the EAPC of ASDR was also observed in Bosnia and Herzegovina (-20.13% (95%CI: -21.76%, -18.47%)) (Figure S1C; Table S4). Chad (958.79 (95%CI: 658.31–1286.7) per 100,000 population) had the highest age-standardized DALY rate in 2019 (Figure S2A; Table S5). DALYs in Chad increased by 112% (95%UI: 39–205%), while deaths in Bosnia and Herzegovina declined by 98% (95%UI: 98–99%) over 30 years (Figure S2B; Table S5). During the same period, Bosnia and Herzegovina (-15.12% (95% CI: -16.89%, 13.31%)) showed the most significant decreasing trend in the EAPC of DALYs (Figure S2C; Table S5). In 1990, Chile had the lowest ASIR at 207.3372 (95%UI: 153.0–281.12) per 100,000 population. Ethiopia (5569.06 (95%UI: 4202.62–7310.2) per 100,000 population) and Bolivia (5250.99 (95%UI: 3909.47–6829.99) per 100,000 population) had the highest ASIRs in 1990 (Figure S3A; Table S3). Ethiopia also had the largest ASDR at 35.04 per 100,000 (95%UI: 26.28–47.66) in 1990 (Figure S3B; Table S4). And the highest age-standardized DALY rate were observed in Timor-Leste (1537.44 (95%UI: 1033.28–2053.91) per 100,000 in 1990 (Figure S3C; Table S5).
Overall, the burden of abortion and miscarriage exhibited a decreasing trend at the global level. Among the 204 countries and territories assessed in 2019, Ethiopia, Niger, and Chad had heavy abortion and miscarriage burdens.
Trends of ASIRs, ASDRs and age-standardized DALY rates by sociodemographic index (SDI)We performed a statistical analysis by SDI. Compared to that in 1990, the disease burden in 2019 was lower in each SDI quintile. In 2019, the largest ASIR was in low-SDI at 1983.8 (95%UI: 1519.8–2558.48) per 100,000 population, while the high-SDI had the lowest ASIR 502.02 (95%UI: 404.72–618.15) per 100,000 population (Fig. 2A; Table 1). In 2019, the ASIR in the low-middle-SDI was 1075.64 (95%UI: 805.82–1390.98) per 100,000 population, which was very close to the global level of 1098.36 (95%UI: 843.01–1391.51) per 100,000 population (Table 1). The ASDRs were lower than the global level at 0.5(95%UI: 0.41–0.59) per 100,000 population in four SDI quintiles, except in the low-SDI (3.03(2.47–3.73) per 100,000 population) in 2019 (Fig. 2B; Table S1). The low-SDI recorded the highest ASR of DALY among all SDI quintiles in both 1990 (684.62 (95%UI: 571.18–815.38) per 100,000 population) and 2019 (165.56 (95%UI: 134.76–201.11) per 100,000 population) (Fig. 2C; Table S2). Low-SDI had the highest age-standardized prevalence (ASPR) both in 1990 (22.67 (95%UI: 14.47–33.39) per 100,000) and 2019 (16.32 (95%UI: 10.43–24.11) per 100,000) (Fig. 2D)., In 2019, the age-standardized YLL rate had significantly decreased across all SDI quintiles compared to 1990, with high-SDI having the lowest age-standardized YLL rate at (0.35 (95%UI: 0.3–0.41) per 100,000 population (Fig. 2E). Low-SDI had the highest age-standardized YLD rates in both 1990 (2.45 (95%UI: 1.3–3.94) per 100,000) and 2019 (1.78 (95%UI: 0.94–2.87) per 100,000) (Fig. 2F).
Fig. 2
Trends of ASIRs, ASDRs and age-standardized DALY rates by sociodemographic index (SDI). The age-standardized incidence (A), death (B), DALY (C), prevalence (D), YLL (E), YLD (F) rate of abortion and miscarriage by year (1990 and 2019). Trends in the number of incidence (G), death (H), DALY (I), prevalence (J), YLL (K), YLD (L) cases of abortion and miscarriage from 1990 to 2019. DALY: disability-adjusted life-year; YLL: year of life lost; YLD: year lived with disability
From 1990 to 2019, most SDI levels showed downward trends in incident cases, with the exception of the low-SDI (Fig. 2G). The most significant decrease in deaths occurred in the low-middle SDI, with a reduction of 19,030 people (Fig. 2H; Table S1). The most significant decline in DALY was also seen in the low-middle SDI (Fig. 2I). The slight increase in prevalent cases was observed in low-SDI from 1990 to 2019 (Fig. 2J). Low-SDI was also had the highest YLLs over the 30 years (Fig. 2K). Additionally, an increasing trend in YLDs was seen in low-SDI during this period (Fig. 2L).
Trends of ASIRs, ASDRs and age-standardized DALY rates in the 21 GBD regionsIn 2019, eastern Sub-Saharan Africa had the highest ASIR (2735.44 (95%UI: 2065.94–3542.31) per 100,000 population), while North America had the lowest ASIR (359.47 (95%UI: 305.88–424.06) per 100,000 population) (Fig. 3A; Table 1). Eastern Sub-Saharan Africa (16.04(95%UI: 12.79–20.29) per 100,000 population) had the highest ASDR in 1990, but Central Sub-Saharan Africa (3.96 (95%UI: 2.88–5.29) per 100,000 population) had the highest ASDR in 2019. The lowest ASDR in 2019 was observed in Australasia, with 0.00156 (95%UI: 0.00118–0.00205) per 100,000 population (Fig. 3B, Table S1). High-income Asia Pacific (0.46 (95%UI: 0.28–0.69) per 100,000 population) had the lowest age-standardized DALY rate in 2019 (Fig. 3C; Table S2). Eastern Sub-Saharan Africa had the highest ASPR in 2019 (22.51(95%UI: 14.37–33.58) per 100,000 population) (Fig. 3D). Central Sub-Saharan Africa had the largest age-standardized YLL rate at 207.38(95%UI: 152.42–273.31) per 100,000 population in 2019 (Fig. 3E). Eastern Sub-Saharan Africa (2.45 (95%UI: 1.28–3.97) per 100,000 population) also had the highest age-standardized YLD rate in 2019 (Fig. 3F).
Fig. 3
Trends of ASIRs, ASDRs and age-standardized DALY rates in the 21 GBD regions. The age-standardized incidence (A), death (B), DALY (C), prevalence (D), YLL (E), YLD (F) rate of abortion and miscarriage compared between 1990 and 2019. Trends in the number of incidence (G), death (H), DALY (I), prevalence (J), YLL (K), YLD (L) cases of abortion and miscarriage from 1990 to 2019. DALY: disability-adjusted life-year; YLL: year of life lost; YLD: year lived with disability
Over the past 30 years, eastern Sub-Saharan Africa showed the largest increase, followed by western Sub-Saharan Africa, while East Asia had the greatest decline (Fig. 3G). Deaths dropped most notably in South Asia, with Southeast Asia next (Fig. 3H). For DALYs, South Asia experienced the sharpest decline over the 30 years (Fig. 3I). Eastern Sub-Saharan Africa also had the greatest rise in prevalence (Fig. 3J). The largest drop in YLLs was in South Asia (Fig. 3K). For YLDs, the most obvious decreasing trend occurred in East Asia, and the most obvious increasing trend was in eastern Sub-Saharan Africa from 1990 to 2019 (Fig. 3L).
Trends of ASIRs, ASDRs and age-standardized DALY rates in different income regionsWe further analysed abortion and miscarriage burden by income level using the Commonwealth and World Bank classifications from the GBD 2019 study. In both systems, low-income area had the highest ASIRs in 1990 and 2019, while high-income area had the lowest (Fig. 4A). Similarly, low-income countries also showed the highest age-standardized rates for deaths, DALYs, prevalence, YLLs, and YLDs, whereas high-income area had the lowest rates (Fig. 4B–F).
Fig. 4
Trends of ASIRs, ASDRs and age-standardized DALY rates in different income areas. The age-standardized incidence (A), death (B), DALY (C), prevalence (D), YLL (E), YLD (F) rate of abortion and miscarriage by year (1990 and 2019). Trends in the number of incidence (G), death (H), DALY (I), prevalence (J), YLL (K), YLD (L) cases of abortion and miscarriage from 1990 to 2019. DALY: disability-adjusted life-year; YLL: year of life lost; YLD: year lived with disability
From 1990 to 2019, the World Bank upper middle-income countries showed the greatest decline in incident cases (Fig. 4G). Deaths in the lower middle-income group exceeded those in the low-income group until 2009, after which the low-income group reported the highest death numbers (Fig. 4H). After 1998, prevalent cases in upper middle-income areas dropped below those in lower middle-income area (Fig. 4J). High-income countries consistently had the lowest YLLs over the three decades (Fig. 4K). A sustained decline in YLDs was observed only in the World Bank upper middle-income areas (Fig. 4L).
Trends of ASIRs, ASDRs and age-standardized DALY rates by age groupWe extracted data from people aged 15–44 years and divided them into six age groups: 15–19, 20–24, 25–29, 30–34, 35–39, and 40–44 years. Compared to 1990, the numbers of incident cases, deaths, and DALYs were lower in all age groups in 2019 (Fig. 5A-F). We found that the 20–24 years group had the largest number of incident cases in both 2019 (13,341,611(95%UI: 8,819,863–18,764,757)) and 1990 (1,028,981(95%UI: 706,394–1,550,370)), suggesting the importance of prenatal screening in younger women (Fig. 5A and D). The number of incidences was the lowest in the 40–44 years (1,352,441(95%UI: 951,622–1,985,526)), but the number of deaths was high in 2019 (3239(95%UI: 2,598–3,988)) (Fig. 5B). We also observed the heaviest DALYs among those females aged 20 to 24 years in 2019 (190,785(95%UI: 155,903–233,177)) (Fig. 5C). In 1990, the 15–19 years group (180(95%UI: 149–219)) had the least number of deaths (Fig. 5E). The 20–24 years group (677,573(95%UI: 548,039–833,442)) had the greatest number of DALY cases in 1990, which may be related to the poor medical treatment (Fig. 5F). The prevalences, YLLs and YLDs are shown in Supplemental Fig. 4.
Fig. 5
Trends of ASIRs, ASDRs and age-standardized DALY rates by age group. The populations were divided into six age groups: 15–19 years, 20–24 years, 25–29 years,30–34 years,35–39 years, 40–44 years. The number of incidence (A), death (B), DALY (C) cases of abortion and miscarriage by age groups in 2019. The number of incidence (D), death (E), DALY (F) cases of abortion and miscarriage by age groups in 1990. The proportion (%) of the six age groups in the total incidence cases (G). The proportion (%) of the six age groups in the total death cases (H). Trends in the number of incidence (I), death (J), DALY (K), prevalence (L), YLL (M), YLD (N) cases of abortion and miscarriage by six age groups from 1990 to 2019. DALY: disability-adjusted life-year; YLL: year of life lost; YLD: year lived with disability
In 2019, the highest proportion of incident cases occurred in the 25–29 years group in countries among high-middle SDI (29.17%), such as Australasia (26.67%). And the 20–24 years group had the largest proportion of incident cases in the low-SDI (32.69%) and low-middle SDI (36.72%), including countries like Central Latin America (35.24%) and South Asia (39.15%) (Fig. 5G). Regarding the total number of deaths, the proportion of people aged 35–39(18.81%) and 40–44(19.49%) is higher globally in 2019 (Fig. 5H).
From 1990 to 2019, incident cases declined in the 15–19, 20–24, and 25–29 age groups, with the 20–24 years group showing the fastest decrease. In contrast, cases gradually increased in the 30–34, 35–39, and 40–44 groups. The 15–19 and 30–34 years groups had equal numbers of incident cases in 2014, afterward, the 30–34 years group had a greater number of cases than the 15–19 years group (Fig. 5I). During this period, deaths decreased across all age groups, with the most significant decline in the 20–24 group (Fig. 5J). DALYs also dropped, especially in the 25–29 years group (Fig. 5K). After 2014, the prevalence in the 30–34 years group was greater than that in the 15–19 years group (Fig. 5L). Although the 25–29 years group showed a general downward trend, it had a greater number of YLLs than the other groups each year (Fig. 5M). In addition, the number of YLDs in the 20–24 years group decreased fastly (Fig. 5N).
Risk factors for abortion and miscarriageAccording to data collected by the GBD 2019 study, iron deficiency is a subclass of child and maternal malnutrition in the behavioural risk category. From 1990 to 2019, global ASDR of abortion and miscarriage due to iron deficiency declined. Among SDI quintiles, the low-SDI had the highest ASDR at (0.7(95%UI: 0.24–1.19) per 100,000 population) in 2019 (Fig. 6A). Among the 21 GBD regions, deaths from iron deficiency significantly decreased, with western Sub-Saharan Africa (0.91(95%UI: 0.31–1.58) per 100,000 population), central Sub-Saharan Africa (0.84(95%UI: 0.3–1.47) per 100,000 population) and eastern Sub-Saharan Africa (0.56(95%UI: 0.2–0.95) per 100,000 population) showing the highest ASDRs in 2019 (Fig. 6B). In 2019, low-income countries had the highest ASDRs, while high-income countries were the lowest (Fig. 6C).
Fig. 6
The death burden attributable to risk factor (iron deficiency) for abortion and miscarriage. A The age-standardized death rate (ASDR) of abortion and miscarriage attributable to iron deficiency globally and in five SDI quintiles in 2019. B The age-standardized death rate (ASDR) of abortion and miscarriage attributable to iron deficiency in 21GBD regions in 2019. C The age-standardized death rate (ASDR) of abortion and miscarriage attributable to iron deficiency in different income areas in 2019. D Trends in the number of deaths of abortion and miscarriage attributable to iron deficiency globally and in five SDI quintiles from 1990 to 2019. E Trends in the number of deaths of abortion and miscarriage attributable to iron deficiency in 21GBD regions from 1990 to 2019. F Trends in the number of deaths of abortion and miscarriage attributable to iron deficiency in different income areas from 1990 to 2019. The proportion of the six age groups for iron deficiency-related deaths globally (G), and in high (H), high middle (I), middle (J), low middle (K), and low SDI quintiles (L) in 2019
Globally, deaths due to iron deficiency dropped rapidly, with the sharpest decline in the low-middle SDI group (Fig. 6D). From 1990 to 2006, the number of deaths in western Sub-Saharan Africa showed an upward trend, surpassing the number of deaths in eastern Sub-Saharan Africa by 2002, and the number of deaths in western Sub-Saharan Africa decreased after 2007 (Fig. 6E). Low-income had more higher numbers of deaths in 2019 (Fig. 6F).
We selected the global level and five SDI quintiles to examine the temporal trends in deaths due to iron deficiency by age group. Overall, the proportion and number of deaths declined in all age groups globally and across the five SDI quintiles from 1990 to 2019 (Fig. 6). The 15–19 years group exhibited the lowest total number of deaths per year (Fig. 6G). Among SDI quintiles, the high-SDI had the most rapid decrease and consistently had the lowest death counts (Fig. 6H). In high-middle SDI, deaths were lowest in the 15–19 group, followed by the 40–44 group (Fig. 6I). The distribution of deaths among the age groups in the middle-SDI exhibited a similar pattern to that in the high-middle-SDI, but the number of people in each age group was approximately 5 times that in the high-middle-SDI (Fig. 6J). Low-SDI had the highest death counts across all age groups and showed relatively minor change over time (Fig. 6K).
The correlation between the SDI and the age-standardized rate of abortion and miscarriageWe investigated the association between the SDI and the age-standardized rate of abortion and miscarriage. Negative correlations were observed between the SDI and the ASIR (ρ = -0.567; P < 0.001) or the ASDR (ρ = -0.724; P < 0.001) (Fig. 7).
Fig. 7
The correlation between the sociodemographic index (SDI) and the age-standardized rate of abortion and miscarriage for 21 GBD regions, 1990–2019. A Age-standardized incidence rate (ASIR). B Age-standardized death rate (ASDR). Lines in the same colour and pattern represent the age-standardized rate of a region, each point in a line represents 1 year starting at 1990 and ending at 2019. The black line represents the average expected relationship between SDI and age-standardized rates for abortion and miscarriage, according to values for each geographic region from 1990–2019
From 1990 to 2019, ASIR generally declined with increasing SDI. Despite a sharper ASIR drop in low-SDI like eastern Sub-Saharan Africa, the disease burden remained high (Fig. 7A). In contrast, ASIR was consistently low in high-SDI, such as high-income North America and the Asia-Pacific (Fig. 7A). ASDR also declined in many regions, with Sub-Saharan Africa showing both the highest ASDR and a decreasing trend as SDI rose (Fig. 7B). However, ASDR remained largely unchanged in some middle- and high-SDI, including Central Europe, Australia, and high-income North America (Fig. 7B).
Comments (0)