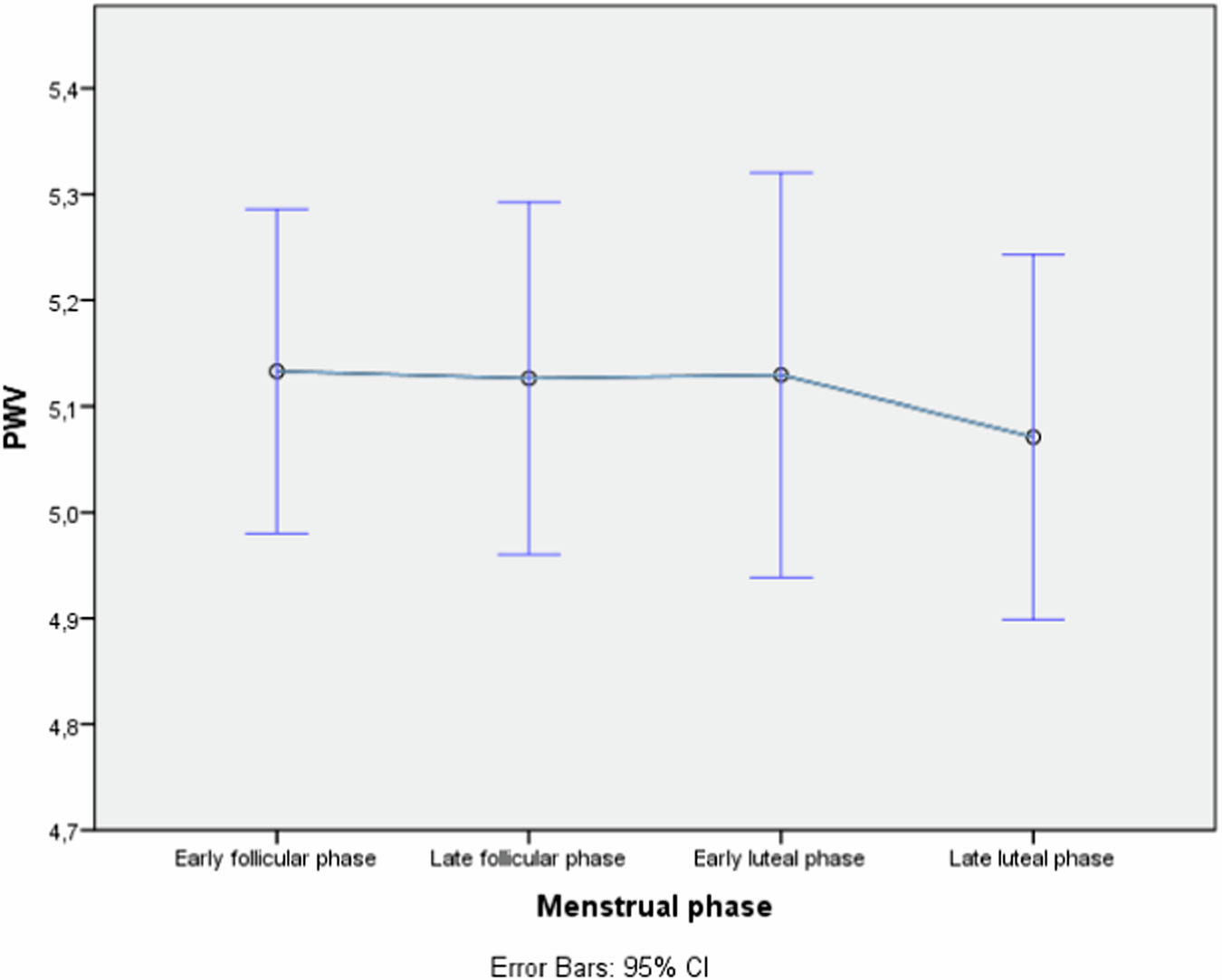
In this study we found a significant association between use of hormonal contraceptives and PWV as a marker of arterial stiffness, but no effect on cIMT and a non-significant trend on AIx. The association between PWV and CP use remained significant after adjustment for established cardiometabolic risk factors BMI, age, blood pressure and SHBG. SHBG, included here as a marker of androgenicity, was strongly dependent on contraceptive use and contraceptive modes of administration (Table 1), and on the subgroup of oral contraceptive used (Table 2), but had only a limited impact on the association between PWV and contraceptive use (Tables 4 and 5). Furthermore, we found no statistically significant difference in PWV and AIx between OCP and PCP groups (Table 1). However, it should be noted that the PCP group was much smaller in our material, reflecting the fact that OCP use is more prevalent among Swedish women. The subgroup analysis of the four the most common oral contraceptives did not show statistically significant mean differences in PWV, AIx or cIMT, which, while a lower power of this analysis merits consideration, could reflect that varying doses of ethinylestradiol and the different kinds of gestagens in the various contraceptives have a limited impact compared to the overall effect of CP treatment compared to non-users. As for the menstrual phases, no differences in PWV were observed (Fig. 1).
With respect to OCP and arterial stiffness, our findings concord with those of Hickson et al. [10] and Yu et al. [11], who found an increased arterial stiffness in their OCP groups. Furthermore, like them, we found no significant association between menstrual phase and arterial stiffness, although our cross-sectional study design is not optimal for assessing this particular factor. Our results with respect to PWV differ from those of Priest 2018 [12] and Enea 2021 [13]. Furthermore, Enea et al. observed, in their study on 49 healthy women, a statistically significant increase in AIx in the OCP group that they stated was difficult to explain in light of the non-significance of PWV in their study. The lack of concordance between PWV and AIx in both our material and that of Enea, while possibly related to measurement sensitivity differences between the two measures, random error or a lack of power, could also be a sign that, while both measurements aim at addressing “arterial stiffness”, they in fact probably correspond to slightly different properties, at different scales, in different parts of the arterial tree [17, 18].
Our study is the first, to our knowledge, to measure arterial stiffness in a PCP group, which displayed significantly higher PWV values than non-CP users. A tendency towards higher PWV in the subcutaneous and vaginal contraceptive groups could be observed (Table 1), however, it should be noted that PCP users were in the minority, and results should be interpreted with caution. While PCP bypass first pass metabolism in the liver, permitting lower dosages than what is typically found in OCPs, pharmacokinetic studies have observed increased plasma concentrations of estrogen in PCP compared to OCP [19]. OCP intake may also be less consistent, with OCP users displaying a lower compliance than parenteral methods [20]. Furthermore, PCPs have been found to confer a greater risk of thromboembolism than OCP [21]. The nature of the differences in CVD risk between OCP and PCP is unknown. Ethinyl-estradiol could play a role, being found in OCPs, but typically not as often in PCP, while both contain progestins. However, we found no differences in vascular measurements between the groups using gestagen only OCP vs those using estrogen containing OCP. At the same time, both estrogens and progestins have been implicated in hypertension, by means of the activation of the renin-angiotensin-aldosterone system (RAAS), altered endothelial function, and oxidative stress [22, 23]. While the exact mechanisms behind the effects are unknown, the contraceptive using group in our material indeed displayed significantly higher CVD risk markers than the non-users; blood pressure, LDL, triglycerides and non-HDL cholesterol were all higher (Table 2).
In this population of young, healthy women, the contraceptive using group, both OCP and PCP, showed increased CVD risk markers, such as a higher lipids and CRP concentration, which concord with the findings of a previous study [24]. The CRP induction caused by orally delivered estrogen has been attributed to the hepatic first-pass effect, not reflecting an increase in systemic inflammation typically associated with an increasing CRP. Nonetheless, our results raise concerns regarding the safety of OCP with respect to arterial health. CRP correlates with endothelial dysfunction [25] and shows a proinflammatory effect on in vitro endothelium [26], which may constitute part of the explanation, but its inclusion in multivariable models (Tables 4 and 5) showed a limited effect on the relationship between contraceptive use and PWV, implying that CRP is only a minor part of the mechanism.
Our study is limited in its cross-sectional design, from which it is not possible to ascertain the order of the alterations in the variables examined. The data collected on contraceptive use is binary and anamnestic and lacks information on the length of hormonal exposure to intake of the contraceptive reported. PWV was measured in triplicate, on one sampling occasion, which did not permit an examination of any differences in PWV in the same individual across the menstrual cycle, nor did it permit an examination of the changes in relation to relation to varying doses over a tablet period in the OCP group. Follow-up studies are warranted that examine the vascular effect in relation to these factors, as well as to the total length of exposure of the contraceptives. The study selection may also not be fully representative of the young female population at large due to the recruitment mode, where the majority of the population was recruited in a university. Future studies are warranted with a longitudinal design, examining the impact of OCP and PCP on stiffness and CVD risk markers on follow-up. The strengths of this study are that all subjects were young healthy non-smokers free of any chronic disorders, and its large population size, in a field of research where previous studies have typically studied small samples (n < 100). This provided us with a higher power to detect even minor differences in the studied variables.
There were statistically significant differences in SHBG between OCP, PCP, and the non-contraceptive using groups (Table 1). This may be related to the differences in androgenicity caused by the different doses of estrogen and gestagens in the different contraceptives used, the length of exposure to these agents, or reflect an effect on the liver from the doses delivered. While androgenicity may also play an important role in CVD risk, SHBG was not independently associated with PWV (data not shown), and the small impact it had as an adjustment variable on our multivariable examinations on the effect of contraceptives on stiffness (Tables 4 and 5) suggests that the relationship between CP use and PWV cannot be attributed to altered androgenicity profiles only.
In conclusion, contraceptive using women exhibited an increased arterial stiffness, measured as PWV, compared to non-users. Despite significant differences in established serum CVD risk biomarkers between NEU or NCU and EU or CU, the inclusion of these biomarkers in adjusted models only moderately affected the association between PWV and contraceptive use, suggesting that an effect exerted by contraceptives on the arterial wall could be caused by direct effects, or by other, yet unidentified, mediating factors. These results merit further study, examining the longitudinal impact of contraceptive use, and the possible mechanisms behind a relationship between contraceptive use and arterial stiffness.


Comments (0)