
Remember me

A total of 9690 patients were included in the trauma registry between 2004–2022 and 2071 patients had an ISS > 15.
A pelvic injury was registered in 2283 patients and 160 of them had an ISS > 15. Men dominated with 115 (72%) and 45 (28%) were women.
Further baseline characteristics are presented in Table 1.
Table 1 Characteristics of patients with severe pelvic trauma treated between 2004–2022Median age of men was 45 years, while women were slightly older at 52 years of age. All 160 patients had a blunt injury mechanism. Transport related injuries were most common with 94/160 (59%) followed by falls (54/160 (34%)). Transport related injuries were most commonly encountered in patients aged < 60 years, while for patients aged ≥ 60 years falls and transport related injuries were equally common.
Transport to hospital was done by ambulance in 83 patients, by helicopter in 75 patients, by a bystander in one case and unknown in one case.
The accidents occurred in 9 different counties with a total of 26 patients injured in counties other than the primary catchment area.
No patients were registered with hypothermia and 17/160 (10%) patients tested positive for ethanol.
DiagnosticsA pelvic x-ray was taken in the trauma bay in 128/160 (80%) patients, with 112 pathological and 21 described as normal. Of these 21 normal x rays, 18 patients went to a CT scan with pathologic findings.
A CT scan including the pelvis was taken in 135/160 (84%) patients with all showing signs of pathology.
Emergency intervention was performed in 33/160 (20%) patients (Table 2). In 27 patients a laparotomy, an EPP or an AE was the primary hemostatic emergency procedure. One patient had an emergency thoracotomy, two patients with severe head injuries had an intracranial pressure monitor and 3 patients had other interventions not specified in the trauma registry.
Table 2 Comparison of injury severity, location of major injury and outcome according to primary hemostatic emergency interventionAll but one EPP were done in the years 2010–2014, with one EPP also performed in 2021. The mortality in the EPP group was very high at 6/8 (75%) while only 1/9 in the laparotomy group succumbed and 2/10 (20%) in the AE group.
Angioembolization was similarly distributed over time as EPP with all but one procedure done in the years 2009–2014, with one procedure in 2017.
Comparison of injury severity, treatment and outcome for the three time periods are presented in Table 3.
Table 3 Comparison of injury severity, treatment and outcome in period 1–3Multiple emergency proceduresFourteen of the patients who had an emergency procedure, had more than one procedure done.
The most common combination was a laparotomy + EPP, which was seen in nine patients, where 2 of these patients also had an adjunct AE.
One of the patients who had an initial laparotomy also had an AE.
Two patients had a laparotomy, EPP and thoracotomy, and one of these also an adjunct AE.
One patient had a thoracotomy followed by an EPP in the emergency room.
Five of the patients who had a laparotomy had ongoing abdominal bleeding that were stopped with hemostatic sutures and packing.
In total 3 patients had a thoracotomy as part of the emergency hemostatic surgery.
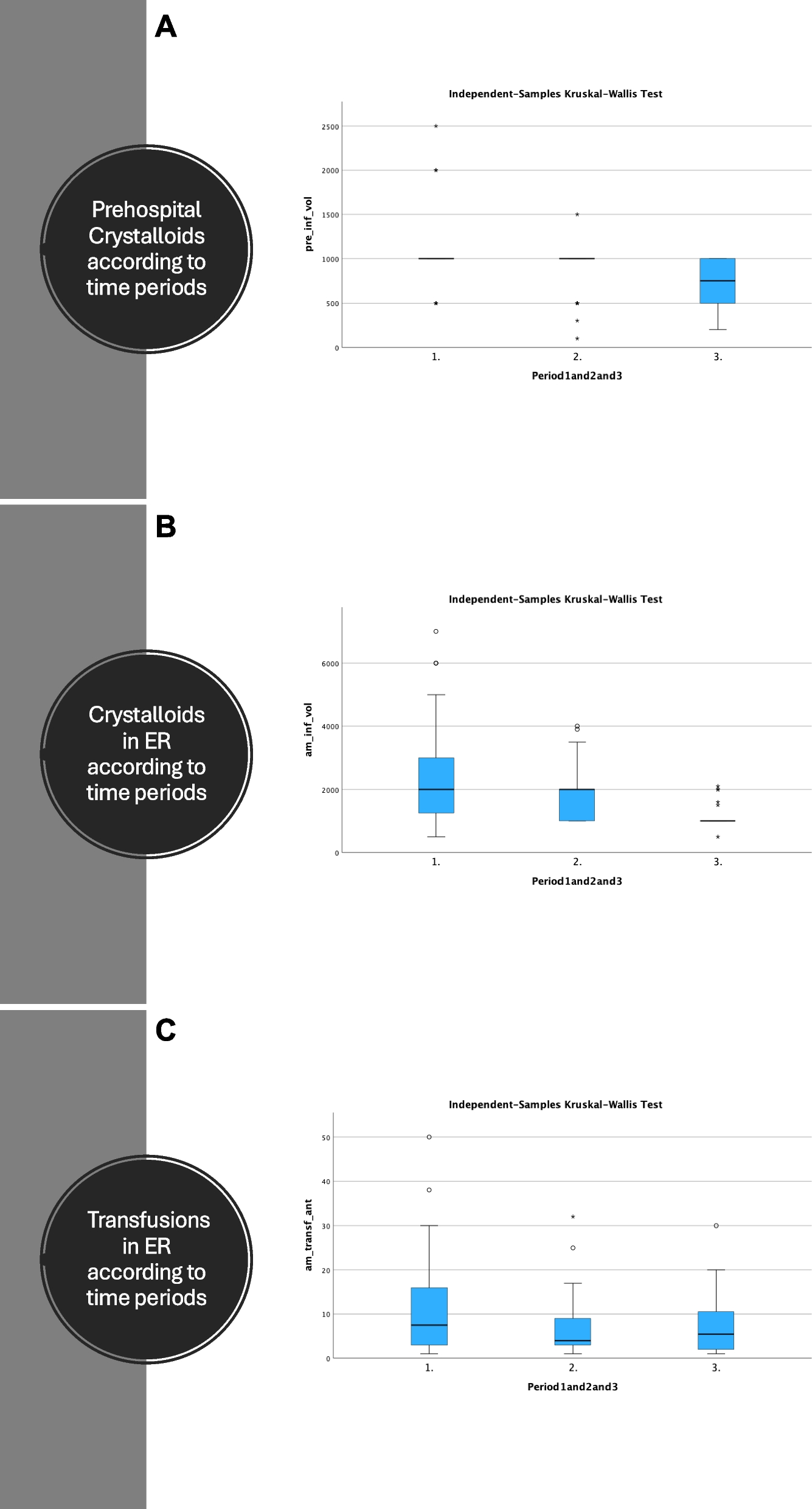
Crystalloids and transfusionsA statistically significant decline in frequency and amount of crystalloids given were seen from period 1 to 3, while the amount of blood transfusions administered in the ER remained stable over time (Fig. 1 panel A-C).
Fig. 1
Panel A Prehospital crystalloids according to time periods. B Crystalloids administered in ER according to time periods. C Transfusions in ER according to time periods
MortalityNo difference in mortality was seen between the three time periods.
A cut off point of 35 years of age had a sensitivity of 80% for mortality by ROC analysis. Figure 2 panel A-E shows ROC curves and area under the curve for factors associated with 30-day mortality.
Fig. 2
Panel A ROC analysis of the association between ISS and Mortality of severe pelvic injuries. Panel B ROC analysis of the association between GCS and Mortality of severe pelvic injuries. Panel C ROC analysis of the association between Age and Mortality of severe pelvic injuries. Panel D ROC analysis of the association between RTS and Mortality of severe pelvic injuries. E ROC analysis of the association between Triss score and survival of severe pelvic injuries
The mortality increased from 13% in those aged 35 and younger to 26% in those aged > 35 years of age. Further, the mortality increased for each decade to 32% for those aged > 50, 35% in those aged > 60, 43% in those aged > 70 and 67% in those aged > 80 years of age.
Three patients were > 90 years of age and they all died.
Univariate analysis and multivariable regression analysis of factors associated with mortality is presented in table S1 and table S2 (supplementary).
A TRISS score < 0.22 had a sensitivity of 0.98 for 30-day mortality by ROC analysis with an area under the curve of 0.91 (figure).
Causes of death are presented in Table 4, where 3 deaths occurred after 30 days.
Table 4 Cause of death in patients with severe pelvic injuries according to time periodsOnly one death occurred in patients without polytrauma.
Comments (0)