Although current guidelines [3, 4] recommend a 7–14 day antibiotic treatment for uncomplicated GNB-BSI, our large cohort found no statistically significant difference in terms of 30-day mortality or relapse within 90 days among hematological patients who underwent short-course (median duration of 8 days) versus prolonged-course (median duration of 14 days) antibiotic therapy. Furthermore, our findings did not establish a correlation between the administration of carbapenem-containing therapies or combination therapies and a reduction in 30-day mortality among patients with non-CRE and ESBL-E BSI. Notably, monotherapy with BLBLI exhibited non-inferior efficacy compared to carbapenem in the treatment of non-CRE BSI, encompassing those infections caused by ESBL-E pathogens. Consequently, based on our observations, we posit that short-course antibiotic therapy and the employment of carbapenem-sparing BLBLI regimens represent viable and effective therapeutic options for hematological patients with non-CRE and ESBL-E BSI.
Several retrospective studies [16, 17] and RCTs [5,6,7] indicated that short-course and prolonged-course antibiotic therapy had a similar survival outcomes. However, the ideal treatment duration for hematological patients is unclear, as they are often excluded from these trials due to their immunosuppressive status. Research on immunocompromised populations was limited. Ranganath et al. [18] studied 206 neutropenic patients with GNB-BSI, including 39 cases of Enterobacteriaceae BSI treated with short-course therapy. There were 11 short-course treatments among 27 episodes of BSI, all of which had composite endpoints (mortality and recurrence within 90 days). A significant difference was not found between prolonged and short-course treatments (hazard ratio (HR) 1.20; 95% CI 0.52–2.74). Furthermore, 82.1% of patients in this study received antibiotic prophylaxis for neutropenia. Recent researches indicated that this practice does not enhance survival [19] and may increase drug resistance [20]. Nonetheless, it is plausible that antibiotic prophylaxis may provide additional, unequivocal antimicrobial coverage post-treatment, thereby potentially influencing outcomes to some extent. And the limited event rate and small sample size constrain the ability to determine the impact of treatment duration on prognosis. A retrospective comparative study of Metais et al. [21] involved 71 AML patients experiencing a total of 104 episodes of BSI. Of these episodes, 43 were attributed to Gram-negative pathogens, and only 8 patients experienced recurrent BSI episodes within 30 days. Among these recurrent cases, antibiotic treatment duration did not appear to be associated with the risk of relapse in five patients who underwent short-course antibiotic treatment (p = 0.37). It is important to note that the propensity score (PS) adjustment in this study did not include all variables that could potentially influence treatment duration. Therefore, there is the possibility that some prognostic and confounding variables were not considered in this study, highlighting some limitations. Our study was meticulously designed to address the previously identified gap in knowledge by enrolling an adequate sample size of hematological patients. In particular, patients who either succumbed to their illness or encountered other events before completing their antibiotic regimen were excluded from the study to mitigate the risk of immortal time bias. In order to minimize potential confounding effects, patients receiving antibiotic treatment outside this pre-defined range were excluded from the study. By adhering to these criteria, we have minimized potential biases and confounding factors, thereby enhancing the generalizability and applicability of our findings to real-world clinical settings.
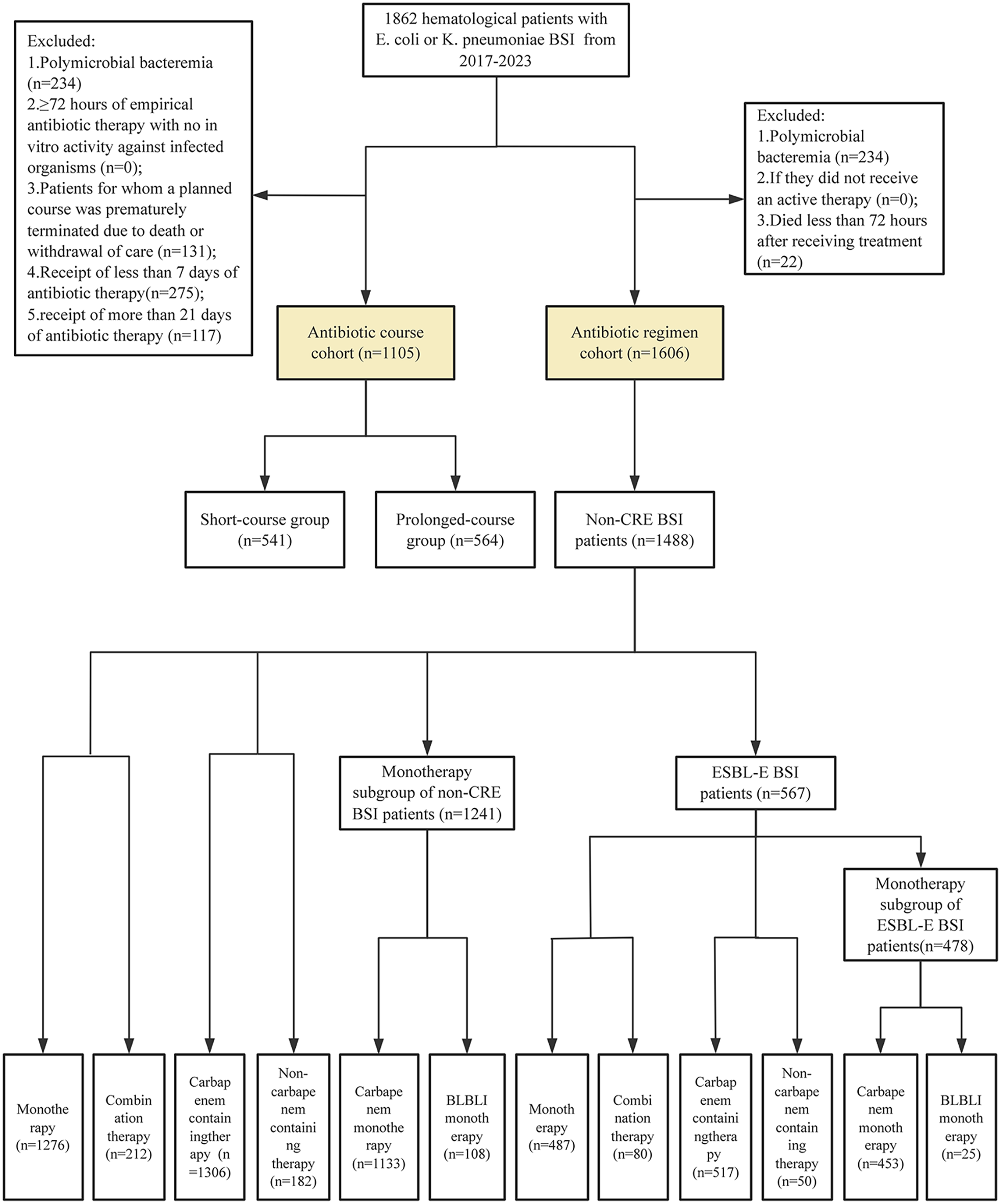
Among hematological patients with ESBL-E and non-CRE BSI, including those with less severe infections such as urinary tract infections, carbapenems emerged as the primary antibiotic choice. Within our antibiotic regimen cohort, 212 non-CRE BSI patients received combination therapy, with 173 (81.60%) receiving carbapenem-based combination therapy. Additionally, 1276 non-CRE BSI patients were treated with monotherapy, of which 1133 (88.79%) received carbapenem monotherapy. In the subset of 567 patients with ESBL-E BSI, 80 patients received combination therapy, with 64 (80%) of these receiving carbapenem-based combination therapy. The remaining 487 ESBL-E BSI patients were treated with monotherapy, of which 453 (93.02%) received carbapenem monotherapy. According to the IDSA [22], carbapenem monotherapy should be used as the first-line treatment for ESBL-E BSI, based on results from MERINO trial [13], which compared the efficacy of BLBLI with carbapenems. Nevertheless, several issues persist within the MERINO trial that may elevate the risk of adverse outcomes in the BLBLI-treated group. For instance, ESBL production is defined based on insensitivity to ceftriaxone without confirmatory testing. Additionally, MICs of all strains were determined by strip tests, which might overestimate the sensitivity of strains to PTZ, reducing its perceived efficacy for treating ESBL-E infections. According to a recent secondary analysis [23] of the MERINO trial, after excluding non-sensitive strains, treated with PTZ did not significantly differ from carbapenems in 30-day mortality. However, the study had a significant proportion of patients with urinary tract infections (over 50%), while immunosuppressed patients constituted less than 30%, and those with neutropenia or hematological malignancies comprised less than 10% of the cohort. In a retrospective study, Gudiol et al. [24] involving 251 hematological malignancies patients with ESBL-E BSI, and found comparable 30-day mortality rates between BLBLI (mainly PTZ) (5.8%) and carbapenems (15.8%) treatment groups in the definitive treatment phase (p = 0.99). However, the sample size was significantly reduced after PSM, leaving only 15 patients in each treatment group. A retrospective study [25] analyzed 180 patients with non-urinary bacteremia caused by ESBL-E, and reported that 30-day mortality in the BLBLI-treated group (11.1%, 7/63) was similar to that in the carbapenem treated group (11.6%, 5/43) (p = 0.926) after PSM. There was a relatively low proportion of patients with hematological malignancies (less than 8%) and undergoing immunosuppressive therapy (less than 20%) in this study. CSL is one of the most frequently utilized BLBLIs in China; however, there is a paucity of outcome studies evaluating its efficacy. Our study encompassed all hematological patients, including both adult and pediatric patients, and had similar outcomes reported by Gudiol et al. We included patients who received antibiotics for more than three days and excluded those who succumbed to their infection within the early stage (less than three days) as well as those with polymicrobial bacteremia, in order to minimize the confounding effects of patient-specific variables or multiple microorganisms. In our clinical setting, CSL is the most commonly prescribed BLBLI for ESBL-E BSI. PSM was employed to balance the confounding factors between the treatment groups. Based on our findings, the use of carbapenem-sparing BLBLIs, such as CSL, in patients with non-CRE and even ESBL-E BSI appears to be feasible.
There were several limitations to our study, primarily due to its retrospective design. The incidence of Clostridium difficile infections, for instance, which would be important to compare between short- and prolonged-course treatment groups, was not reported. Furthermore, although we employed strict inclusion and exclusion criteria to enhance the evaluation of outcomes and mitigate immortal time bias, it may limit the generalization of our research results to a range of immunosuppressed patients. Despite the utilization of PSM and multivariate analysis to mitigate selection bias and potential confounding factors, the influence of unmatched confounding variables may still persist.
In summary, the results of this study indicate that short-course antimicrobial treatment does not lead to poor prognosis or recurrence in hematological patients with E. coli or K. pneumoniae BSI, and may offer the added benefit of facilitating earlier hospital discharge. Furthermore, combination therapy was not associated with a reduction in 30-day mortality, and carbapenem-sparing antibiotic regimens had non-inferiority to carbapenem in non-CRE BSI patients, even in BSI caused by ESBL-E. These results provide evidence for appropriate antibiotic stewardship in the two most prevalent bacteremia encountered in hematological patients, which warrant clinicians to reduce carbapenems use. However, it remains essential to undertake randomized controlled trials to furnish additional evidence and validate these findings.

Comments (0)