To the best of our knowledge, this research stands as one of the relatively few studies to delve into lithium-induced hypothyroidism over an extended duration, documenting both the prevalence and incidence of this condition over a decade. Notably, the initial year of lithium therapy marked a substantial decline in survival rates from hypothyroidism. Furthermore, we were able to pinpoint younger age, presence of physical illness, and higher serum lithium levels as key associated factors for lithium-induced hypothyroidism. Our findings underscored the low incidence of hypothyroidism, indicative of the overall safety of long-term lithium usage, while also identifying specific risk factors that warrant clinical attention in select populations.
The incidence of lithium-induced hypothyroidism in our study closely aligns with findings from some previous studies [5, 11]. When comparing our results to the Whickham Survey, a seminal UK study on thyroid disorder incidences in a community setting, where annual hypothyroidism rates were reported as 0.41% in women and 0.06% in men [14], our observed rates of 2.75% in women and 1.57% in men were notably higher. Our examination of survival rates indicated a significant decrease in the initial year, similar to the results seen in Lazarus et al. [6], yet occurring earlier than in a separate study where a considerable percentage displayed abnormal TSH levels after 3 years (91.4%, affecting 19.9% of all patients) as identified by Duce et al. [15].
While previous research has often identified female sex as a significant risk factor for lithium-induced hypothyroidism [11, 16], we did not observe any differences in prevalence, incidence, or survival rates between female and male patients in our study. However, our findings align with a recent study as noted by Almadani et al. [17]. The considerable disparities in reported prevalence, incidence, and associated factors of lithium-induced hypothyroidism in previous studies can be attributed to the heterogeneity of criteria employed and the study populations’ characteristics regarding factors such as sex ratio, geographical origins of patients, iodine intake, and the proportion of subjects with autoimmunity [5, 11].
In our study, we discovered that older age acted as a protective factor against hypothyroidism in patients undergoing long-term lithium therapy. With each year of increasing age, the odds of developing lithium-induced hypothyroidism decreased by 5% (adjusted OR = 0.95, 95% CI = 0.92,0.98, p = 0.001). Shine et al. [2] also found the greatest risk of developing lithium-induced hypothyroidism among younger women. Interestingly, we did not observe an association between the age at which patients commenced lithium therapy and lithium-induced hypothyroidism. It is worth noting that in previous studies, initiating lithium therapy above the age of 50 was significantly linked to higher odds of lithium-induced hypothyroidism [3, 5]. Our findings also revealed that older patients were more likely to receive higher doses of lithium carbonate, implying that they may have been thoroughly screened and deemed physically robust by their psychiatrists before opting for lithium as part of their treatment. Further investigation is warranted to validate these findings.
This study indicated a correlation between physical illnesses and an increased likelihood of developing lithium-induced hypothyroidism. These medical conditions or accompanying treatments might elevate the risk of thyroid malfunction. Currently, there is limited concrete evidence to fully substantiate this association. For instance, Shine et al. [2] identified that patients with diabetes mellitus faced a heightened risk of lithium-induced hypothyroidism (HR = 1.08, 95%CI = 1.05–1.12, p < 0.0001). Previous research has suggested that insulin resistance, hyperglycaemia, and leptin levels influence serum TSH levels [18]. Both diabetes mellitus and thyroid dysfunction can have an autoimmune origin, and these autoimmune diseases often cluster within individuals, indicating a shared pathophysiological basis or genetic predisposition [19, 20]. Nonetheless, based on our encouraging results, individuals with such physical conditions should undergo regular thyroid function monitoring.
Strengths and weaknesses of the study
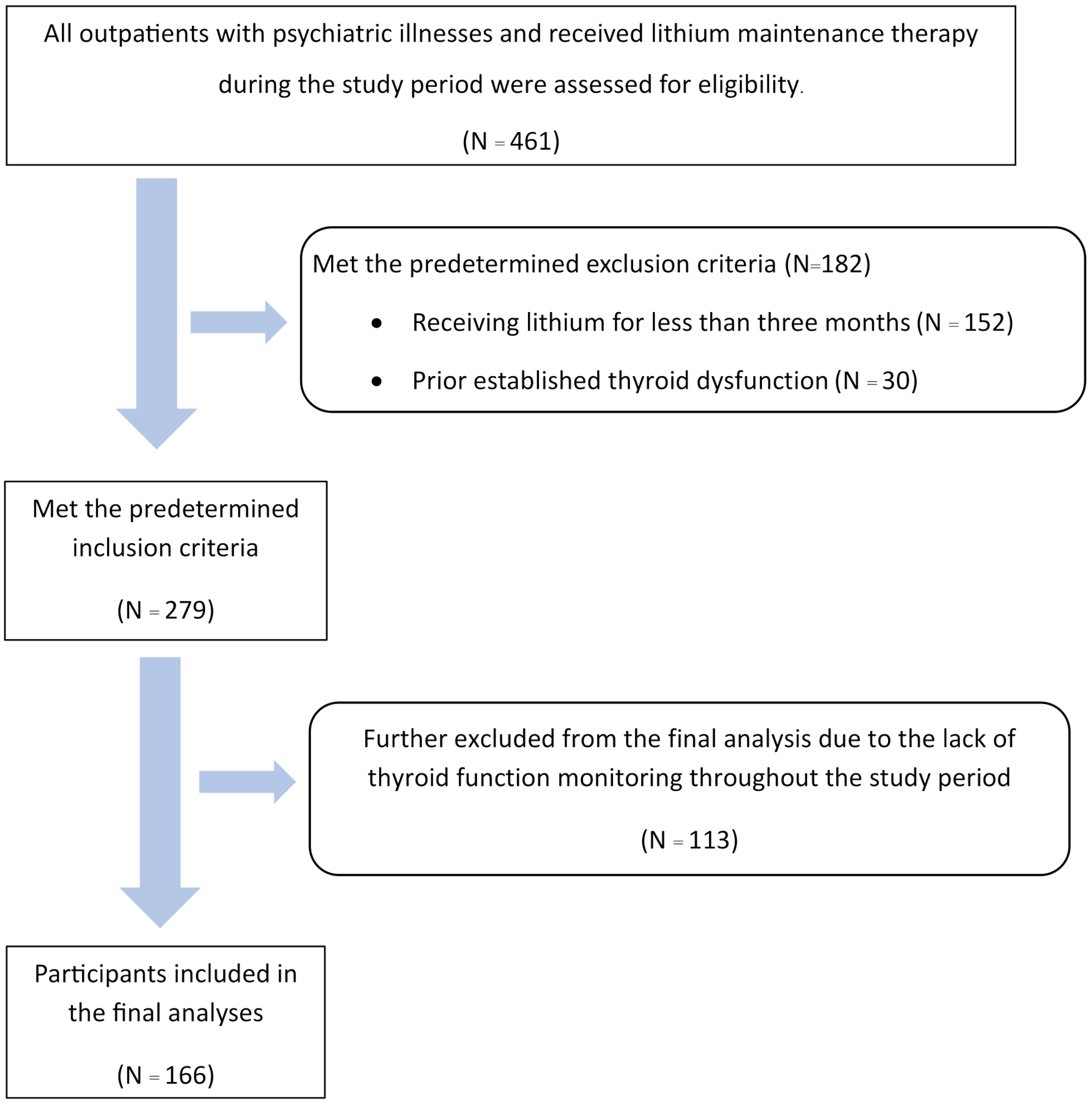
While our study meticulously examined the medical records of patients undergoing long-term lithium therapy over the past decade, several limitations need to be acknowledged. Firstly, the retrospective nature of the study hindered the establishment of causal relationships. Notably, approximately 41% of patients on long-term lithium therapy did not undergo thyroid function monitoring, potentially leading to an error in the estimation of the incidence of lithium-induced hypothyroidism. Moreover, thyroid antibody presence and a positive family history of hypothyroidism have been recognised as significant risk factors for lithium-induced hypothyroidism [21, 22]; however, these factors were not routinely assessed or documented in the medical records we reviewed. Consequently, the absence of such data in our analysis could have confounded our results.
Clinical and research implications
We found that many long-term lithium therapy patients were not consistently monitored for serum lithium levels and thyroid function, especially if they were younger and on lower lithium doses. Despite the low incidence, thyroid dysfunction can occur in individuals with low serum lithium levels [23]. Our study also noted that younger patients may face a higher risk of lithium-induced hypothyroidism. It is crucial for clinicians to maintain regular thyroid function checks, even in younger patients on lower lithium doses [23]. While a recent study highlighted potential over-requesting of thyroid function tests in lithium patients, leading to possible over-diagnoses that may self-resolve [15], we still encourage regular thyroid function monitoring. Our study suggested most cases developed abnormal thyroid functions around six months to 4 years (IQR = 5.2,53.2 months), with a median of around one year. In line with our findings, clinicians may endorse adherence to NICE guidelines advocating thyroid function tests every 6 months and more often if there is evidence of impaired thyroid function or an increase in mood symptoms that might be related to impaired thyroid function [24]. Further suggested by our findings, those with physical comorbidities and higher serum lithium levels may also warrant more vigorous surveillance of hypothyroidism.
In our study, we pinpointed several risk factors that can aid in prioritizing resources for screening and assessing lithium-induced hypothyroidism. While challenging due to the condition’s rarity, a large prospective cohort study is essential to comprehensively gather covariates for a more in-depth understanding. Such a study would facilitate improved prevention, detection, and treatment strategies for lithium-induced hypothyroidism.

Comments (0)