Baseline Characteristics
Seventy patients with FD were treated at our institution during the study period. Of these, 41 (21 males, 20 females) underwent at least one DXA scan: 19 patients had one scan, 11 had two scans, 9 had three scans, and 2 had four scans. A comparative analysis revealed no significant differences between patients who underwent DXA scans and those who did not, with respect to: age, sex, and disease severity, as assessed by FuSS scores, balance, and BARS.
The median age at the first DXA scan was 25 years (range 7–47); 14 patients were younger than 20 years. The median age at the last follow up was 32 years (range 12–53). Clinical characteristics, anthropometric measurements and laboratory results of the cohort are presented in Table 2. Seven patients were treated with antiepileptic drugs, three with anti-depressive drugs, 11 with fludrocortisone and 15 with proton pump inhibitors.
Table 2 Clinical characteristics, laboratory tests and anthropometric measurements at the first dual energy X-ray absorptiometry scan of 41 patients with familial dysautonomiaDisease Severity and Ambulation
The median scores (interquartile range) for the FuSS, balance, and BARS are presented in Table 2. FuSS scores ranged from 25 to 48. Six patients (15%) score between 25 and 30, 24 patients (58%) scored between 31and 40, and 11 patients (27%) scored between 40 and 48.
The balance scores ranged from 1 to 5. Two patients (5%) had a score of 1, seven patients (17%) had a score of 2, nine patients (22%) had a score of 3, 12 patients (29%) had a score of 4, and 11 patients (27%) had a score of 5.
BARS scores ranged from 0 to 29. Twenty-five patients (60%) had scores between 0 and 10, 13 patients (32%) had scores between 11 and 20, and three patients (8%) had scores between 21 and 29.
Regarding ambulation, one patient required a wheelchair for mobility, eight patients (20%) could ambulate unassisted only at home, and 31 patients (77%) were able to ambulate unassisted for more than 100 m.
BMD and TBS
BMD and TBS measurements at the first DXA scan are presented in Table 3. A BMD Z-score below − 1 was observed in 50–91% of patients, depending on the measurement site. A BMD Z-score below − 2, which is considered the lower limit of the normal range for age [26], was found in 22–70% of the patients. The mean TBS Z-score was − 1.8 ± 1.6, significantly lower than expected in a healthy population (p < 0.01).
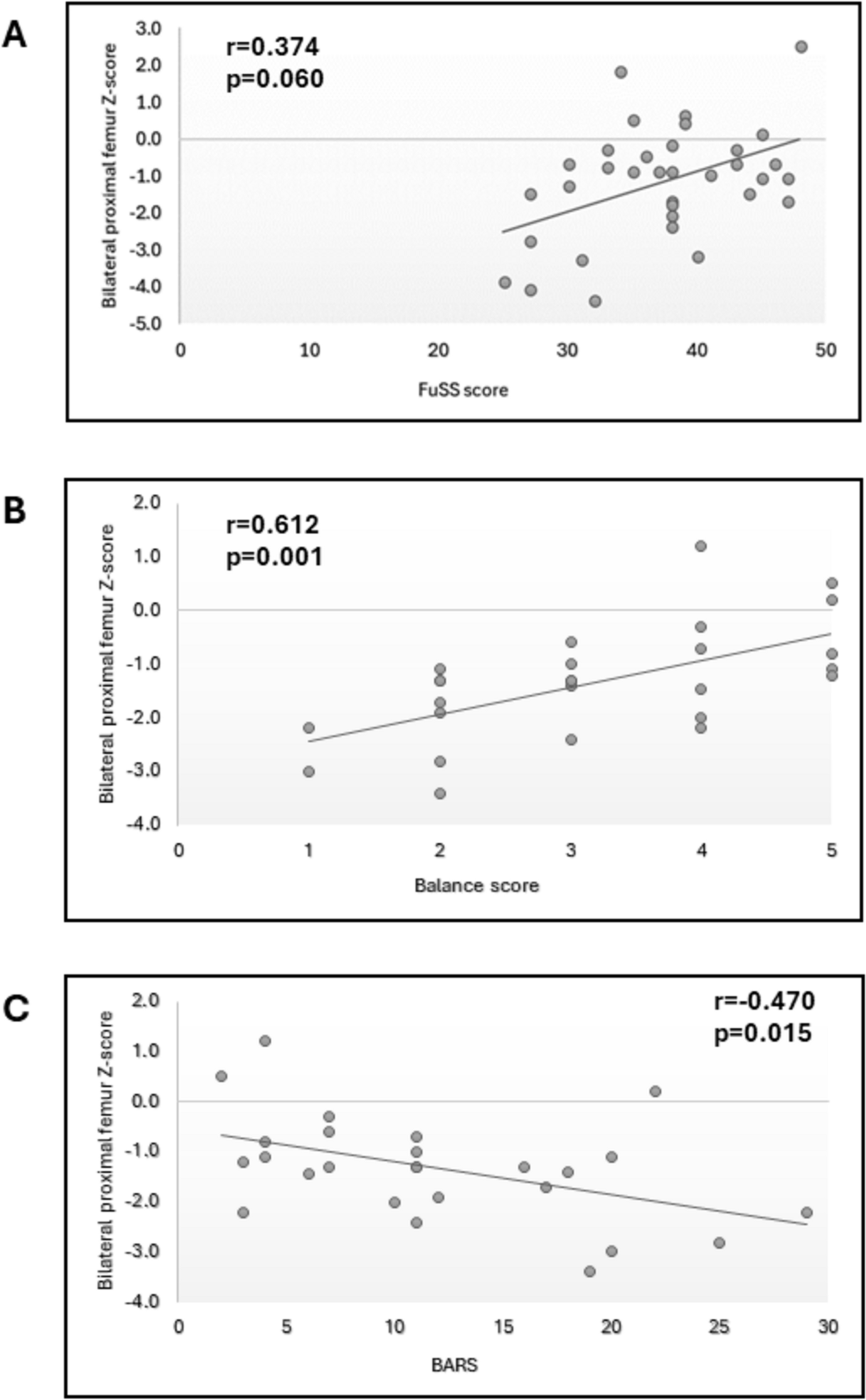
Table 3 Bone mineral density and trabecular bone score at the first dual energy X-ray absorptiometry scanWe found significant correlations between BMD and disease severity. Lumbar spine and TBLH Z-scores were correlated with better scores of FuSS (r = 0.451, p = 0.007 and r = 0.674, p = 0.016, respectively). Left femoral neck, right femoral neck and bilateral proximal femur scores were correlated with better scores of balance, BARS and ambulation ability (Table 4). The third radius Z-score was correlated with better scores for balance (r = 0.518, p = 0.011), FuSS (r = 0.410, p = 0.05) and the ataxia scale (r = − 0.498, p = 0.016).
Table 4 Correlations of bone mineral density of the femurs with the Functional Severity Scale (FuSS), balance, ambulation and the Brief Ataxia Rating Scale (BARS)The L1–4 Z-score was also positively correlated with the height Z-score (r = 0.398, p = 0.02) and weight Z-score (r = 0.393, p = 0.021). The TBLH Z-score was positively correlated with the height Z-score (r = 0.696, p = 0.012), weight Z-score (r = 0.889, p < 0.001) and BMI Z-score (r = 0.613, p = 0.034).
We did not find correlations of BMD with levels of calcium, phosphorous, vitamin D and parathyroid hormone levels.
Bone Turnover Markers
The values of P1NP and CTX of 15 patients are presented in Table 5. Ten (67%) patients had CTX above the normal range, and three (20%) had high P1NP. Among those aged > 16 years, CTX and P1NP were negatively correlated to L1–4 Z-scores (r = − 0.681, p = 0.03 and r = − 0.700, p = 0.02, respectively). We also found negative correlations of CTX and P1NP with FuSS (r = − 0.515, p = 0.10 and r = − 0.619, p = 0.042, respectively). Accordingly, higher CTX and P1NP levels were correlated to worse disease severity.
Table 5 C-terminal telopeptides of type I collagen (CTX) and procollagen type I N-terminal propeptide (P1NP) values of 15 patients with familial dysautonomiaFractures
At the time of the first DXA scan, 20 patients (49%) reported at least one past fracture. Eleven patients had one fracture, two had two fractures, three had three fractures and four had four fractures. Distribution of fractures by anatomical site is presented in Table 6. Patients with or without fractures did not differ significantly in bone density measurements, TBS z-scores, FuSS score, ataxia scale and ambulation.
Table 6 Distribution of fractures by anatomical site in familial dysautonomia cohortLongitudinal Follow Up
Twenty-two patients had two consecutive measurements of BMD of the bilateral proximal femur. The mean time lapse between the first and last scans was 4.0 ± 2.4 years. The mean BMD Z-score at this site was − 1.3 ± 0.9 at the first scan, and − 1.5 ± 0.9 at the last scan (p = 0.043).
Medical Treatment for Bone Health
Twenty-five patients (61%) took calcium supplements and 32 (78%) took vitamin D. Three patients (7%) were treated with bisphosphonates. Two of the latter were treated with bisphosphonates during young adulthood due to low BMD (Z-scores < − 2) and fractures. The third patient received treatment during adolescence. At age 16 years, she was referred by an orthopedic surgeon for bisphosphonate therapy prior to scoliosis surgery. She received three doses of zoledronic acid, and had no significant adverse effects. Notably, her BMD showed substantial improvement. At baseline, the lumbar spine BMD Z-score was − 4.4, and TBLH BMD Z-score was − 3.9. A follow-up DXA scan performed 2.8 years later revealed marked improvement, with a lumbar spine BMD Z-score of − 1.8 and TBLH BMD Z-score of − 1.7. Following this second scan, the patient underwent C5-L4 posterior spinal fusion.

Comments (0)