This study reported patterns of BMD loss following menopause at multiple skeletal sites. During the first five years postmenopause, the rate of bone loss was greater at the lumbar spine and ultra-distal forearm compared to the other two time categories. Bone loss was also more pronounced over time for non-users of HT compared to those who did use HT.
The Vietnam Osteoporosis Study has also reported patterns of femoral neck and lumbar spine BMD loss during the menopause transition [13]. A total of 1062 women were categorised into the following age groups: 40–44 years (premenopausal), 45–49 years (perimenopausal), 50–54 years (early postmenopausal), and 55–59 years (late postmenopausal) and had BMD measured twice, approximately two years apart. The study reported a small amount of bone loss occurred before the age of 45–49 years, followed by a greater decline between 50 and 54 years, which slowed between 55–59 years. Although the categorisation of menopause status was different in this study (based on age categories) compared to our study (based on self-reported menopause age), the results are similar, that a substantial amount of bone loss occurs during the first few years following menopause.
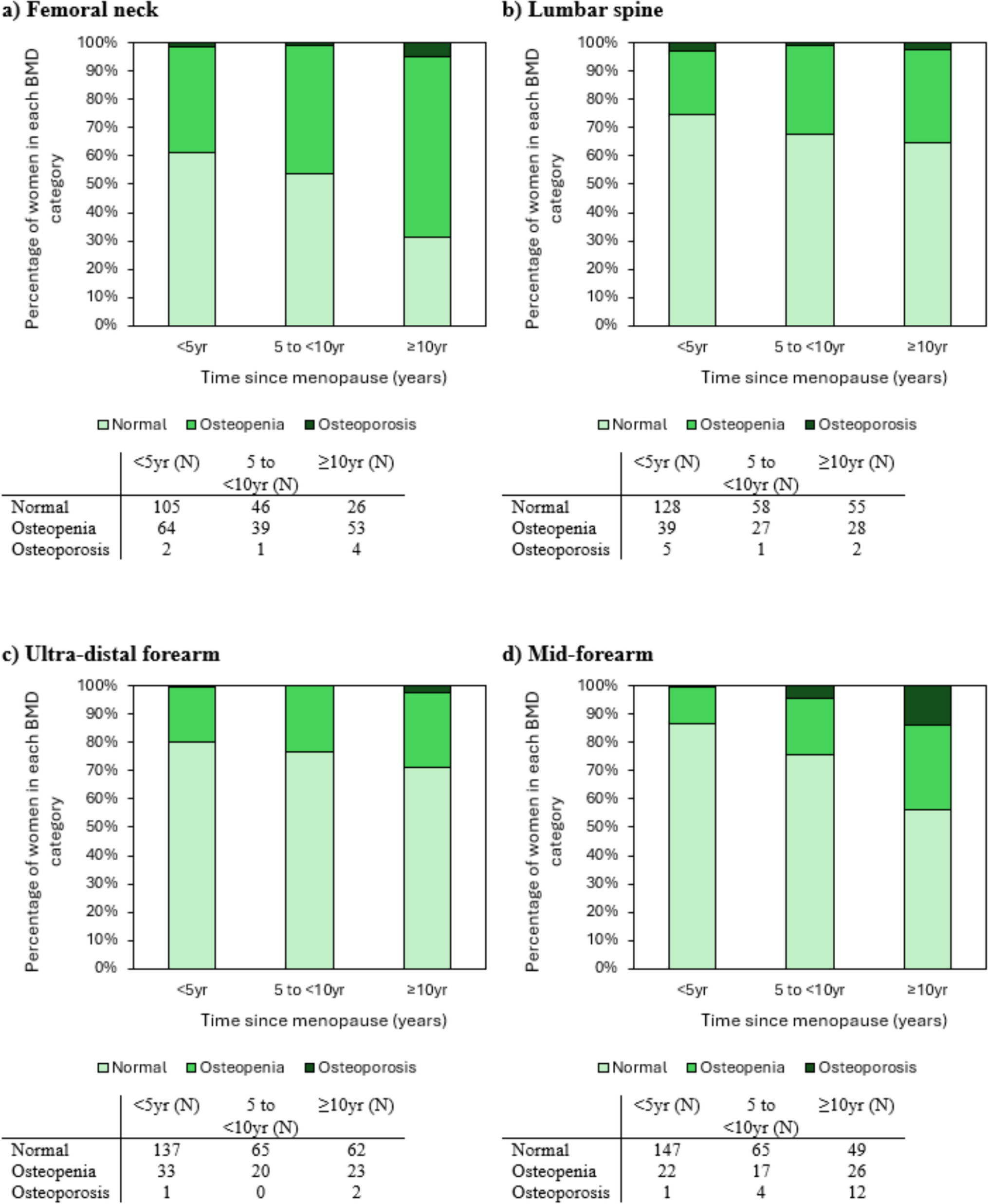
Another study from Iran examined the prevalence of osteopenia/osteoporosis at the femoral neck and lumbar spine among perimenopausal women (2.8 ± 1.5 years since menopause) with a mean age of 49.7 ± 2.0 years [14]. At the femoral neck, it was reported that 35.2% had osteopenia and 8.0% had osteoporosis. For the lumbar spine, the proportions of osteopenia and osteoporosis were 41.6% and 12.0%, respectively. The proportion of women with osteopenia at the femoral neck was comparable to that observed in our study for women within the group < 5 years since menopause (35.2% vs 37.1%). However, other proportions of osteopenia and osteoporosis were lower in our study. This may be due to differences in study population: our participants were population-based and not excluded on the basis of disease, while the Iranian study did have some exclusion criteria. Additionally, in our study, baseline T scores for the femoral neck were lower than at the other sites, which may explain the results. Despite this, both studies report a substantial proportion of women around the time of menopause to have osteopenia at the femoral neck or lumbar spine.
In this study, we reported that the rate of BMD loss was more pronounced during the first five years postmenopause at the sites with a higher proportion of trabecular bone, specifically the lumbar spine and ultra-distal forearm. This may be explained by bone turnover occurring faster in trabecular bone [4]. Other studies have also reported similar results, specifically a higher or similar rate of BMD loss at the lumbar spine, which is a primarily trabecular site, compared to the femoral neck, which contains a higher amount of cortical bone [3, 13, 15, 16]. Additionally, a study by Riggs et al. [9], which used quantitative computed tomography to assess rates of bone loss across the adult age range, reported that trabecular bone loss began in young adulthood, but cortical bone loss did not occur until older ages. Another study by Ó Breasail et al. [17] using peripheral quantitative computed tomography also reported similar results, showing that menopause was associated with lower bone density and strength at the distal radius; a site that contains a significant amount of trabecular bone.
In a longitudinal study by Greendale et al. [5], which included 705 pre- or perimenopausal women, examined changes in trabecular bone score (TBS), which is associated with trabecular microarchitecture, around the time of the FMP. The study reported that TBS began to decline 1.5 years prior to the FMP and this rate increased until approximately two years after the FMP, after which the rate of decline began to plateau.
Although bone loss is faster in trabecular bone, the majority of the skeleton is cortical (80%), and a previous study using high-resolution peripheral quantitative computed tomography (HR-pQCT) has shown that much of the bone remodelling in menopause occurs at sites with higher proportions of cortical bone [4]. The loss of trabecular bone at a specific location stops once the trabecular structure has been fully resorbed. However, for cortical bone, as more is resorbed, a larger surface area for further resorption is created [4]. These results together indicate that the loss of cortical bone during and shortly after menopause, in additional to trabecular bone loss, may be an important determinant of the risk of future fracture.
Another cross-sectional study has examined differences in pQCT-derived bone parameters among 430 women at different stages of menopause (pre-, peri- and post-menopause) [17]. The study reported that later menopause stage was associated with lower bone density and strength at the distal radius (4% site), as well as lower cortical density and thickness at the proximal radius (66% site). The reduction in cortical thickness observed for postmenopausal women supports the findings above, where cortical bone is resorbed, resulting in a reduced cortical thickness.
Previous studies have also examined risk factors for bone loss during the menopause transition. In a longitudinal study of southern Chinese women [16], lower age at menopause, higher baseline age, lower body weight and higher follicle-stimulating hormone concentration were associated with a higher BMD loss at the spine, femoral neck and total hip over a four year follow-up period. Similar results were reported in a Korean study [18] which showed that higher age, higher percent body fat, lower thyroid-stimulating hormone and lower serum uric acid levels were associated with a larger BMD loss at the lumbar spine over a two year follow-up period. Lower body weight and BMI as well as previous fragility fracture were also associated with a faster rate of BMD loss in another study [19] of 50 women aged < 60 years who were followed over 9 years. Targeting those risk factors which are modifiable may be useful in preventing or slowing bone loss during the menopause transition.
In Australia, bisphosphonates are government subsidised under specific conditions including age ≥ 70 years and a diagnosis of osteoporosis [20]. However, by the time a woman meets these criteria, they may have lost a substantial amount of bone and sustained one or more fractures. These women may have benefited from earlier preventative strategies, though additional work is needed to explore the cost-effectiveness and appropriateness of such an approach. It has previously been reported that HT use in postmenopausal women has been associated with a greater BMD and reduced non-vertebral fracture risk [21, 22], indicating a potential role for HT in the maintenance of bone health. The most recent position paper from The National Osteoporosis Guideline Group (NOGG) [23], recommends that HT should only be initiated for the treatment of post-menopausal osteoporosis in younger women (age ≤ 60 years) who have low risk for adverse malignant and thromboembolic events. Additionally, the 2022 version of the Hormone Therapy Position Statement of The North American Menopause Society (NAMS) [24] provides similar recommendations; for women aged < 60 years, within 10 years of menopause and no contraindications, HT has a favourable benefit-to-risk ratio for prevention of bone loss. It is also recommended that ongoing HT use should be discussed after the age of 60–65 years, taking into account the individual’s risks of adverse effects such as cancer, coronary heart disease, stroke, venous thromboembolism, and dementia [23, 24].
This study had several strengths and limitations. A major strength is that we had repeated measures of BMD at multiple sites over a long time period. We were also able to determine which participants were taking HT and stratify the analyses accordingly. Limitations include that menopause data were self-reported; hormone levels were not available at any of the follow-up assessment phases. HT use was updated at each follow-up, allowing ascertainment of the duration of use, however, this may have affected the results for the 5 to < 10 yr and ≥ 10 yr time categories. For example, a participant may have used HT during the first few years following menopause, and then stopped, which may have influenced bone loss during the later time periods post cessation. Additionally, subtle changes in participant positioning for the DXA scans, particularly for the forearm sites, could have occurred over the different assessment phases, which may have affected the resulting BMD measurements. However, at each assessment phase, positioning for the forearm scan was performed using a positioning board, and the participant was asked to make a loose fist with their hand. This was repeated systematically for each measurement, in an effort to reduce errors related to positioning.

Comments (0)