
Remember me
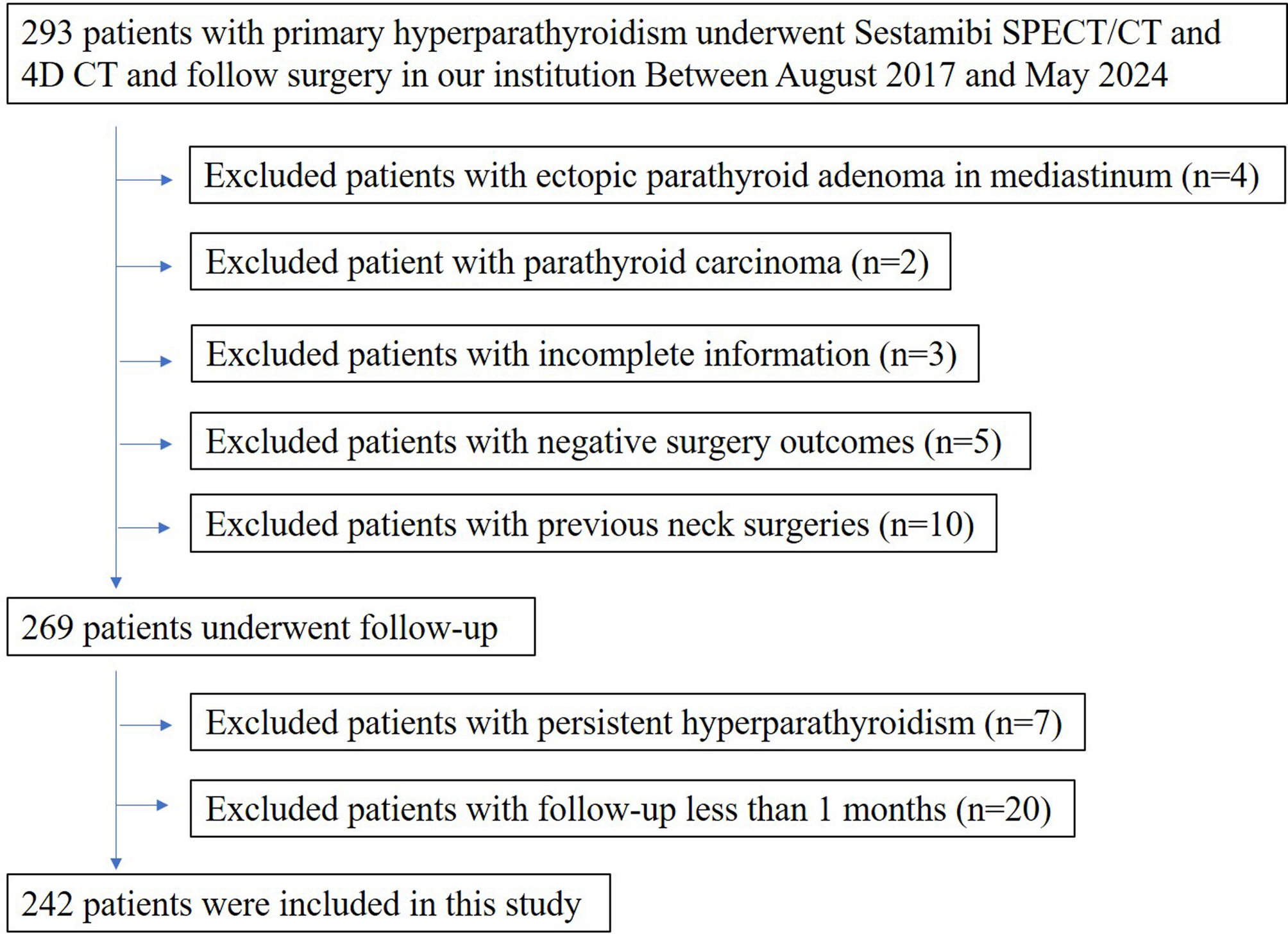
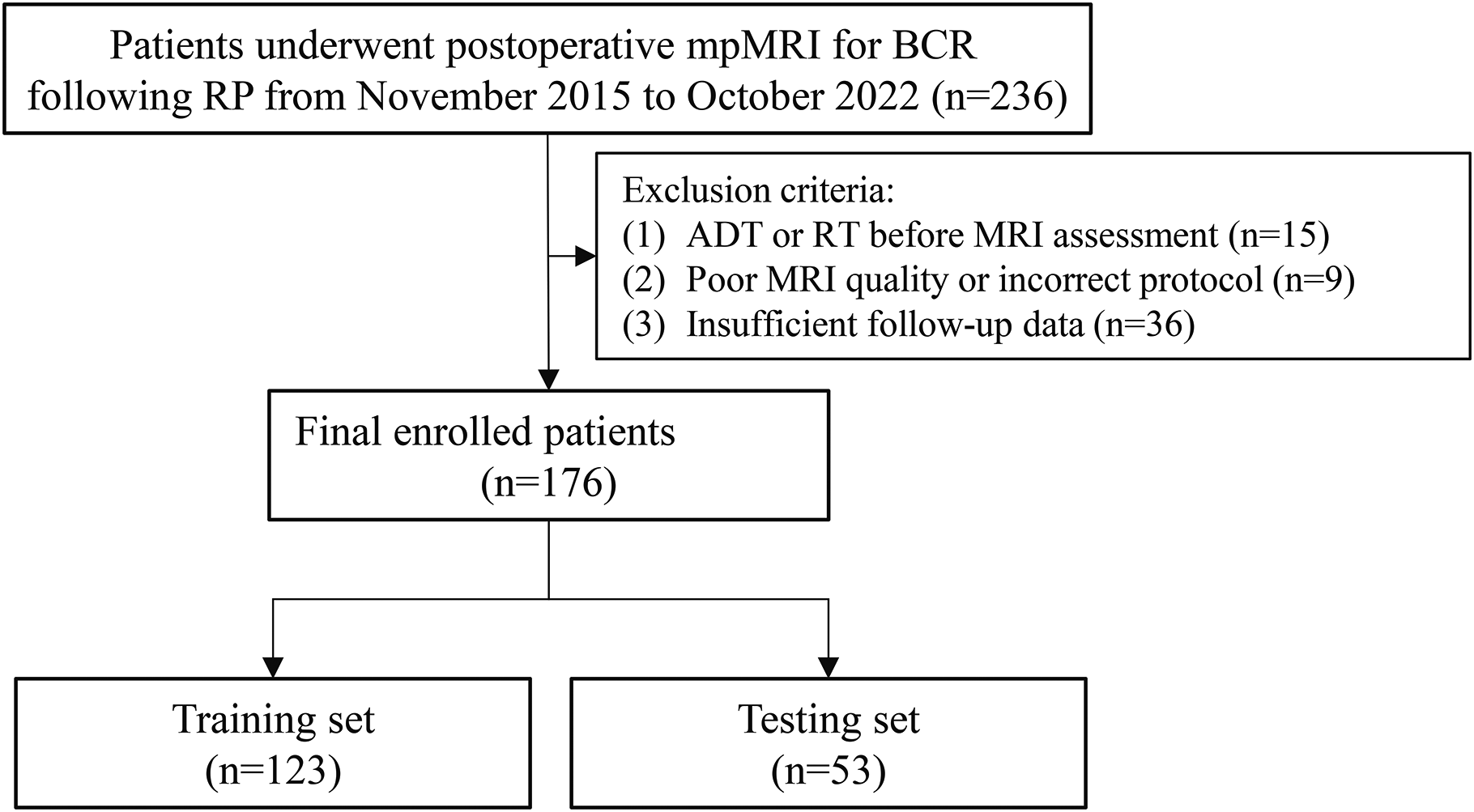
Between August 2017 and May 2024, 293 patients with PHPT underwent a combination of imaging tests followed by parathyroidectomy at our institution. Fifty-one patients were excluded: 10 patients due to a history of thyroid or parathyroid surgery, 3 patients due to incomplete imaging information, 5 patients due to unfavorable surgical outcomes, 7 patients due to persistent hyperparathyroidism, 4 patients due to ectopic parathyroid adenoma, 2 patients due to parathyroid carcinoma, and 20 patients due to being followed up for less than one month. Figure 1 shows the flow of patient inclusion in our study. The clinical and pathological characteristics of the 242 patients (166 females; mean ± SD age: 52.5 ± 13.4; age range: 20–83 years) included in the final analysis are listed in Table 1. The mean calcium, phosphorus and 25-hydroxyvitamin D levels were 2.80 mmol/L (normal, 2.08–2.60), 0.87 mmol/L (normal, 0.85–1.51) and 31.6 ng/mL (normal, 12.3–107), respectively. The median PTH, alkaline phosphate and creatinine levels were 256.4 pg/mL (normal, 12–65), 134.5 U/L (normal, 45–125) and 73.4 µmol/L (normal, 41–97), respectively.
Fig. 1
Study flowchart with consecutive patients with primary hyperparathyroidism and inclusion and exclusion criteria
Table 1 Clinical and pathologic characteristics of patients with primary hyperparathyroidismParathyroid disease characteristics and follow-upA total of 242 patients were assumed to have four parathyroid glands for the four-quadrant analysis (n = 968). Among the 242 patients, 233 patients (96.3%) had single-gland disease, and 9 patients (3.7%) had multigland disease. All 9 patients with multigland disease had double adenomas or hyperplasia. The 251 lesions had a mean (± SD) maximal diameter at pathologic evaluation of 18.6 mm ± 9.2. A total of 120 of 251 (47.8%) were from the left, and 131 of 251 (52.2%) were from the right. The distribution of abnormal glands per quadrant is summarized in Table 1. All patients were followed up for at least one month. The median follow-up time was 6 months (range 1–69 months).
Diagnostic performanceIn 242 patients, 768 parathyroid glands were normal or abnormal according to the per quadrant analysis for the diagnostic performance of each imaging modality. Figure 2; Table 2 show the ROCs for all the modalities and a comparison of the ROCs for both sestamibi SPECT/CT and 4D-CT. The combined-modality sensitive reading and the sestamibi SPECT/CT had the highest ROC, which was not significantly different (p = 0.14) but significantly differed from that of 4D-CT (p = 0.0006). Sestamibi SPECT/CT had a significantly different (p = 0.0006) ROC curve that was greater than the ROC curve of the combined-modality-specific reading. There was no significant difference in the ROC curve between sestamibi SPECT/CT and 4D-CT (p = 0.11).
Fig. 2
Receiver operating characteristic (ROC) curves for sestamibi SPEC/TC (A), 4D-CT (B), combined 4D-CT with Sestamibi SPECT/CT sensitive reading (C), and combined 4D-CT with Sestamibi SPECT/CT specific reading (D) via a per-lesion, four-quadrant analysis
Table 2 Comparison of receiver operating characteristic curveTable 3 summarizes the accuracy, sensitivity, specificity, PPV and NPV of all the modalities. Sestamibi SPECT/CT exhibited an accuracy of 92% (95% confidence interval: 90%, 94%; 891 of 968), similar to that of 4D-CT (91%; 95% confidence interval: 89%, 92%; 876 of 968), combined-modality sensitive reading (91%; 95% confidence interval: 89%, 93%; 878 of 968) and combined-modality specificity reading (92%; 95% confidence interval: 90%, 94%; 889 of 968). The sensitivity of combined-modality sensitive reading was higher than that of sestamibi SPECT/CT (sensitivity, combined-modality sensitive reading vs. sestamibi SPECT/CT: 92% [95% confidence interval: 88%, 95%; 230 of 251] vs. 85% [95% confidence interval: 80%, 89%; 231 of 251]). 4D-CT demonstrated sensitivity superior to that of combined-modality-specific reading (sensitivity, 4D-CT vs. combined-modality-specific reading: 81% [95% confidence interval: 76%, 86%; 204 of 251] vs. 75% [95% confidence interval: 69%, 80%; 287 of 251]). Combined-modality-specific readings were more specific than combined-modality-sensitive readings were (98% [95% confidence interval: 97%, 99%; 702 of 717 and 90% [95% confidence intervals: 88%, 93%; 648 of 717], respectively). Sestamibi SPECT/CT revealed a specificity of 95% (95% confidence interval: 93%, 96%; 678 of 717), similar to that of 4D-CT.
Table 3 Diagnostic performance in the patients with primary hyperparathyroidismSimilar trends were noted in the subset analysis of patients with single-gland disease: the accuracy of sestamibi SPECT/CT was 93% (95% confidence interval: 91%, 94%; 860 of 928), whereas it was 91% (95% confidence interval: 89%, 93%; 842 of 928) for 4D-CT and 92% (95% confidence interval: 91%, 94%; 858 of 928) for combined-modality-specific reading. Similar to the results for all patients, the sensitivity and specificity for all modalities in patients with single-gland diseases ranged from 76 to 93% and 90-98%, respectively.
In patients with multigland disease, 4D-CT had a greater accuracy than sestamibi SPECT/CT (85% [95% confidence interval: 74%, 96%; 34 of 40] vs. 78% [95% confidence interval: 65%, 90%; 31 of 40], respectively) and was similar to the combined-modality sensitive reading (85%, 34 of 40). Compared with sestamibi SPECT/CT, combined-modality sensitive reading had greater sensitivity (79% [95% confidence interval: 60%, 97%; 15 of 19] vs. 63% [95% confidence interval: 41%, 85%; 12 of 19], respectively). Compared with 4D-CT, combined-modality-specific reading had greater sensitivity (47% [95% confidence interval: 25%, 70%; 9 of 19] vs. 32% [95% confidence interval: 11%, 52%; 6 of 19], respectively). Higher specificity was noted for the 4D-CT and combined-modality-specific readings (100%; 21 of 21]) than for the sestamibi SPECT/CT and combined-modality-sensitive readings (90%; 19 of 21). Figures 3, 4 and 5 present examples of the modalities used in patients with single-gland and multigland diseases.
Fig. 3
Images of a 53-year-old woman with primary hyperparathyroidism. Sestamibi SPECT/CT images (A, MIP SPECT; B, axial SPECT; C, fusion SPECT/CT) reveal focal radioactivity uptake localized to a single abnormal right superior parathyroid gland (red arrows). 4D-CT (D, axial noncontrast-enhanced; E, arterial phase; F, delayed phase) showing a vividly enhancing lesion at the arterial phase and washout of contrast material with decreasing attenuation compared with the atrial phase at the delayed phase (red arrows). The patient underwent parathyroidectomy for a single right superior parathyroid adenoma. Normal PTH and calcium levels were observed after 6 months of follow-up
Fig. 4
Image of a 57-year-old man with primary hyperparathyroidism. Axial noncontrast-enhanced CT (A) image showing an oval lesion (red arrows) localized to the right inferior parathyroid gland. Axial sestamibi SPECT image (B) showing focal radioactivity uptake localized to a single abnormal right superior parathyroid gland (red arrow). Axial 4D-CT (C, arterial phase; D, delayed phase) reveals an enhanced right inferior parathyroid gland (arrows) corresponding to the same gland identified via sestamibi SPECT/CT. Additional mild focal radioactivity uptake was noted in the left superior parathyroid gland (yellow arrows) on sestamibi SPECT/CT (E, axial noncontrast-enhanced; F, axial SPECT), which was not obscured on 4D-CT (G, arterial phase; H, delayed phase). The patient underwent bilateral four-gland exploration for left superior parathyroid hyperplasia and right inferior parathyroid adenoma. Normal PTH and calcium levels were observed after 19 months of follow-up
Fig. 5
Image of an 83-year-old woman with primary hyperparathyroidism. Sestamibi SPECT/CT images (A, axial noncontrast-enhanced; B, axial SPECT; C, fusion SPECT/CT) reveal focal radioactivity uptake localized to a single abnormal right inferior parathyroid gland (red arrows). 4D-CT (D, arterial phase; E, delayed phase) shows a vividly enhancing lesion at the arterial phase and persistence of contrast material with increasing attenuation compared with the atrial phase at the delayed phase (red arrows). An additional left superior parathyroid gland (yellow arrows) was observed on noncontrast-enhanced CT (F), which revealed no focal uptake on sestamibi SPECT/CT (G, axial SPECT; H, fusion SPECT/CT), but mild moderate enhancement was noted on 4D-CT (J, arterial phase; K, delayed phase). The patient underwent bilateral four-gland exploration for left superior parathyroid hyperplasia and right inferior parathyroid adenoma. Normal PTH and calcium levels were observed after 26 months of follow-up
Comments (0)