In the present study, we systematically examined the social and psychological phenotype of adult women with TXS. We compared a relatively large cohort of 44 women with TXS to a well-matched control group based on sex, age, and level of education. We assessed key areas including demographic factors, verbal IQ, psychopathology, emotion regulation, coping mechanisms, social anxiety, empathy, and autistic traits. The findings offer a nuanced understanding of their mental health profile, aligning with prior research while also providing novel insights. Beyond group-level comparisons, we examined whether the timing of diagnosis (prenatal vs. postnatal) within the TXS group was related to differences in psychological outcomes. Although no statistically significant differences were found between prenatally and postnatally diagnosed females in our sample, we observed a general tendency toward higher scores of internalizing symptoms (e.g., depression, stress, social anxiety) in the prenatally diagnosed group. This somewhat contrasts with findings by Wigby et al. [50], who reported better overall psychosocial outcomes among prenatally diagnosed females compared to those diagnosed postnatally. Possible explanations for this discrepancy include differences in sample characteristics, assessment methods, or the timing and context of diagnosis. Our results suggest that early diagnosis does not necessarily provide a straightforward protective effect against psychological symptoms. Further studies with larger cohorts are needed to clarify the impact of prenatal diagnosis on mental health outcomes in individuals with TXS.
The lack of significant differences in age and education supports the validity of our matching process. Unlike previous studies, which rarely accounted for education, we matched participants on this factor due to its profound influence on cognitive, social, and psychological outcomes, which may contribute to the differing findings. However, it should be noted that educational attainment is not independent of cognitive and psychological factors and can also be influenced by them. Thus, matching on education may reduce observed group differences by controlling for a variable that partly reflects the outcome itself.
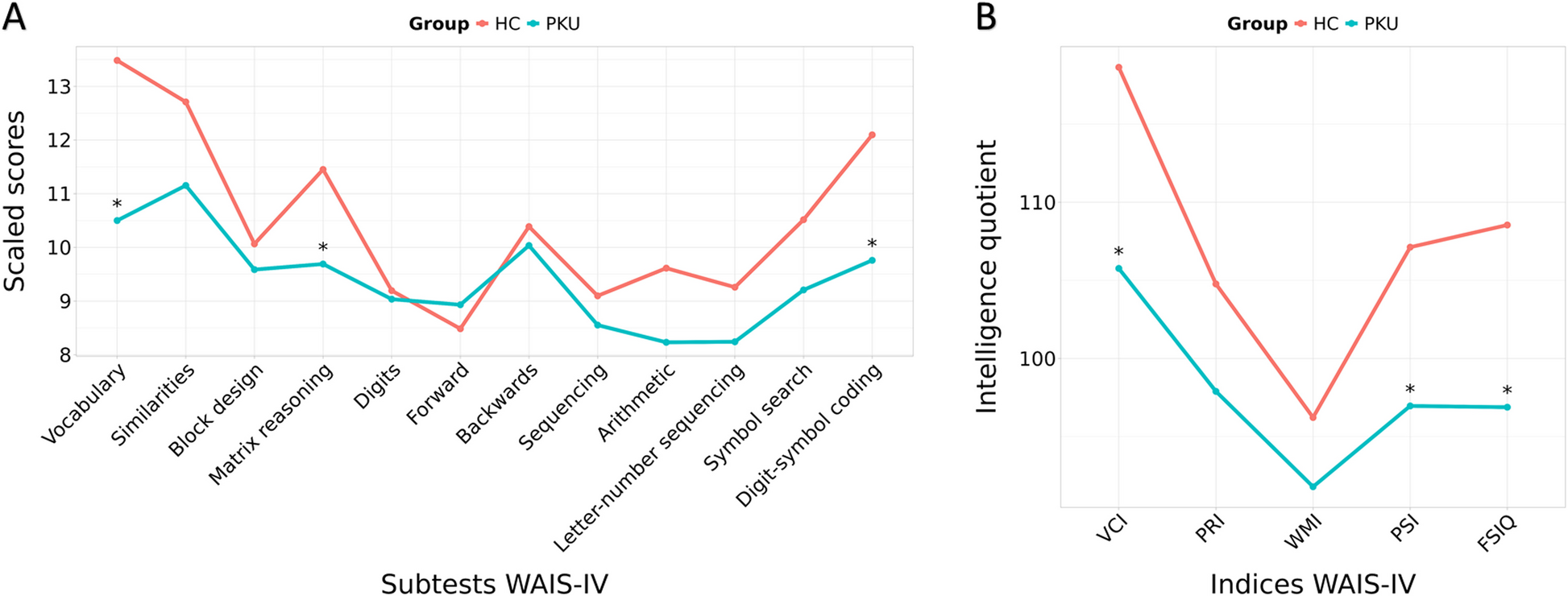
The verbal IQ of both groups was slightly below 100, with no significant difference between the triple X and control groups. This finding contrasts with previous studies that reported reduced IQ scores around 80 to 85 in children, adolescents, and relatively young women with TXS [51,52,53,54,55], indicating mild cognitive impairments. Our results did not show the expected lower verbal IQ in the TXS group, which may partly reflect differences in study design, such as the use of the WST—a simplified method for estimating selectively verbal IQ. However, in a parallel study with a subsample, we used the more comprehensive CFT-20 to measure general intelligence, which yielded similar results [14]. A critical factor that likely contributes to this discrepancy is ascertainment bias. Our sample consisted of adults with TXS who were capable of completing an extensive online self-report battery, suggesting that participants with relatively higher cognitive functioning may have been more inclined or able to participate. This potential selection bias must be taken into account when interpreting the absence of significant group differences in IQ. While differences in sample characteristics—such as age—may also play a role, and while it is conceivable that cognitive deficits seen in childhood might not persist into adulthood, these explanations are more speculative. Furthermore, earlier studies may have captured effects of domain-specific challenges, such as attention difficulties, which are more prevalent in individuals with TXS due to the higher rate of ADHD [22]—a factor we did not assess in our study.
In addition to cognitive and psychological assessments, we also observed distinct patterns in physical health and lifestyle factors. Our results align with previous small studies [51, 56] and the Million Veteran Program study of 61 American women with TXS [15], which reported a taller stature. Unlike the Veteran study, which found no BMI differences and classified both groups as overweight, our study found both groups to have relatively normal weight, with TXS women having a significantly lower BMI. This discrepancy may reflect cultural differences in diet and lifestyle factors. An American study from 1990 noted a tendency toward being underweight in TXS women, which may partly reflect lower BMI levels in the general U.S. population at that time.
The TXS group was more often childless, a finding that aligns with earlier studies noting reduced relative reproductive rate, lower fertility, and increased incidence of premature ovarian failure in women with TXS [2, 16, 57,58,59]. Nearly three times as many women with TXS had at least one physical health condition compared to controls. Prior large-scale studies have identified an increased occurrence of a wide variety of diseases in the TXS population [3, 16]. Our findings reaffirm the heightened health burden in this group and highlight the need for routine medical screening and preventive care in women with TXS.
Additionally, there was a lower prevalence of smoking and alcohol consumption in the TXS group. To the best of our knowledge, apart from the Million Veteran Program Study, which found no significant differences, this aspect has not yet been investigated in TXS. Both alcohol and nicotine use or dependence, respectively, are highly comorbid [60], genetically influenced complex conditions [61] and are generally more prevalent among men than among women [62]. Genes that escape X-inactivation on the X chromosome and are therefore more highly expressed in women with TXS may contribute to phenotypic variability in such traits, though their specific roles remain to be clarified.
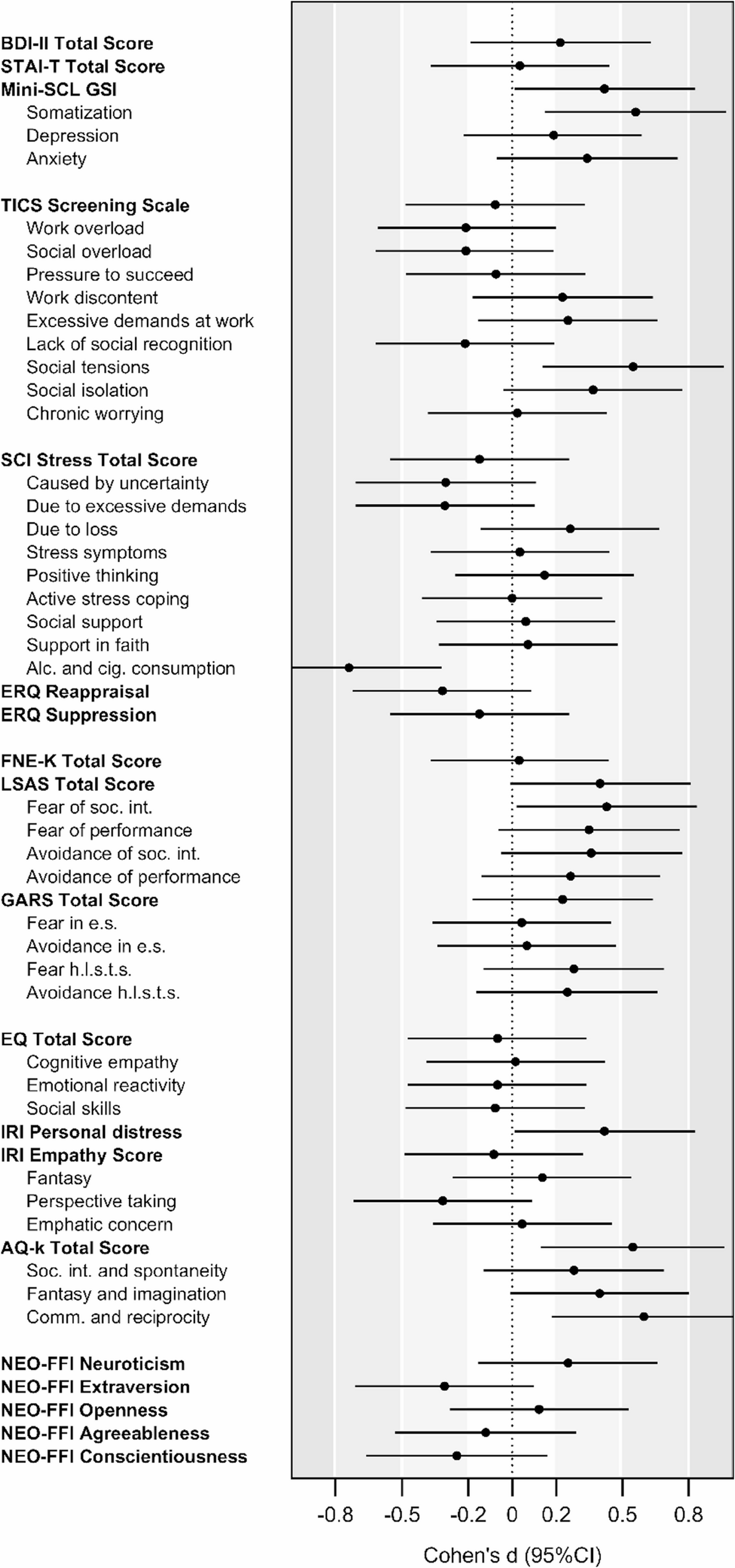
In terms of psychometric assessment, although only cutoff-based categorical comparisons survived correction for multiple comparisons, uncorrected findings are also discussed in relation to their effect sizes, due to their potential relevance. Among these, the TXS group showed higher levels of self-reported autistic traits, particularly in communication and reciprocity, as well as a greater percentage of individuals exceeding the cutoff for a likely clinical ASD diagnosis, both with a medium effect size. Although meeting AQ-k criteria is not equivalent to a clinical diagnosis of ASD, the AQ-k is considered an effective tool for differentiating individuals on the autism spectrum from those with typical development [46]. Our findings corroborate earlier studies indicating elevated rates of ASD in children and young adults with the karyotypes XXX, XXY, XYY, and X [2, 23, 50]. Van Rijn et al. [23] demonstrated that children with an extra X chromosome exhibited fewer autism symptoms than those with ASD but showed increased social anxiety compared to controls, a pattern not observed in ASD children, highlighting differences in social reflective abilities. Similarly, the findings in our adult sample revealed a greater prevalence of likely social anxiety disorder (SAD) in the TXS group, as determined by specific LSAS total score cutoffs. These findings align with prior research indicating impaired social functioning in adult women with TXS [18]. Furthermore, Otter et al. [55] identified a prevalence of generalized anxiety disorder (GAD) of 20.6% in their sample, compared to 3.2% in non-education-matched controls. This aligns with our own prevalence rate of 22.7%, although our controls also showed a relatively high prevalence of 20.0%. As previously discussed, this elevated rate in our control group may be due to education-matching, since social anxiety has also been correlated with lower socio-economic status [63]. Interestingly, there were no significant differences in terms of self-reported fear of negative evaluation and gaze anxiety, both of which are positively correlated with social anxiety [40]. This suggests that while some aspects of social anxiety appear to be elevated in the TXS group, these specific dimensions may not be as strongly affected.
In partial contrast to our initial hypothesis of reduced empathy in TXS—which was based on a previous study on children with TXS [23], we found no significant differences in overall empathy scores or on the IRI subscales “fantasy”, “perspective taking”, or “empathic concern”. However, the TXS group exhibited elevated scores on the subscale “personal distress”, with a moderate effect size. As discussed by Lawrence et al. [43] this subscale is not considered a direct measure of empathy, as it is self-oriented rather than other-oriented, assessing personal anxiety and discomfort when witnessing another’s distress. Personal distress is linked to social withdrawal [64] and social anxiety [65]—traits that, as described above, were observed more frequently in individuals with TXS in our study and in previous research. Additionally, the proportion of individuals classified as having low empathy based on their self-report differed significantly between groups, with nearly three times as many individuals in the TXS group falling below the EQ cutoff compared to controls, with a moderate effect size. This suggests that while group differences may not be apparent in the total empathy scores, a subset of individuals with TXS reports particularly low empathy levels. In contrast to ASD, which is typically associated with deficits in cognitive empathy and, to a lesser extent, affective empathy [55], TXS shows a more varied pattern of empathic traits.
These social difficulties, particularly the elevated rates of social anxiety, autism spectrum traits, personal distress, and reduced empathy are likely contributors to the increased risk of psychological disorders observed in women with TXS in prior studies. In the following section, we will explore the broader emotional challenges faced by this group, focusing specifically on depression, anxiety, somatization, and chronic stress. No significant differences were found for general measures of depression (BDI-II), trait anxiety (STAI-T), or neuroticism (NEO-FFI), contrasting with previous findings reporting elevated symptoms in individuals with TXS [2, 13, 16, 17, 19, 50]. However, scores in both groups were notably high compared to normative mean values reported in manuals or validation studies [27, 29, 47]. Davis et al. [15], in their Veteran Study, found similar results, with no significant differences between groups and a relatively high prevalence of anxiety and depression in both cases and controls, which they attributed to possible effects of military service. Notably, their study also reported similar education levels in both groups, aligning with our study, in which participants were matched for education level.
Depression and anxiety, often grouped as emotional disorders, share etiologies and vulnerability factors such as trait anxiety and neuroticism, which were considered as synonymous by some authors, as both describe a predisposition toward experiencing negative emotions like worry and distress [66, 67]. These elevated scores across both groups may reflect broader societal trends, such as rising emotional distress and disorder prevalence, exacerbated by the COVID-19 crisis [68,69,70]. These trends are particularly pronounced in women, younger individuals, and those of lower socio-economic status—characteristics reflected in our sample. Given that women with TXS often have lower socio-economic status [71], the inclusion of education-matched controls—a rarely implemented approach in prior TXS studies—may partly explain the high scores observed even in the control group.
While no significant differences in psychological distress, as measured by the BDI-II, STAI-T, and the neuroticism scale of the NEO-FFI, were observed, the TXS group showed higher Mini-SCL GSI scores, with a moderate effect size, indicating greater psychological distress, primarily driven by elevated somatization scores. Differences in the sensitivity and focus of different assessment tools may explain these discrepancies, as somatic symptoms are not assessed by the three questionnaires mentioned above. The Mini-SCL results align with earlier research, including our previous study, where increased scores for somatic complaints were also observed [17, 19]. Somatization occurs when individuals express psychological distress through physical symptoms rather than directly experiencing it emotionally. Together, these findings further corroborate the elevated psychological distress in individuals with TXS, highlighting the need for therapeutic interventions aimed at enhancing emotional processing and expression, thereby reducing the reliance on somatic manifestations of distress.
To our knowledge, this is the first study to systematically investigate chronic stress in women with TXS. We examined various facets and sources of chronic stress, as well as coping and emotion regulation strategies, using three diagnostic tools: the TICS, SCI, and ERQ. Notable differences were observed in social tensions, with a medium effect size, as women with TXS exhibited higher scores, highlighting challenges in interpersonal contexts that may contribute to their stress experience. These findings are consistent with prior research indicating that social functioning is a key area of difficulty for individuals with TXS [17,18,19] and further underscore the elevated levels of social anxiety and personal distress identified in this study, emphasizing the significant challenges individuals with TXS face in navigating interpersonal contexts. No significant differences were observed across the remaining TICS and SCI stress subscales, including all work- and performance-related stress scales, suggesting that elevated social stress might be more domain-specific rather than a generalized stress response.
While adaptive coping strategies did not differ significantly between groups, the TXS group demonstrated significantly lower reliance on the maladaptive strategy of alcohol and cigarette consumption, with a medium to large effect size. This finding aligns with the previously discussed lower prevalence of smoking and alcohol use in this group.
Regarding emotion regulation strategies, no differences emerged for either reappraisal or suppression, suggesting that the elevated social stress observed in the TXS group is not necessarily attributable to specific deficits in emotion regulation or adaptive coping strategies. However, it is important to note that self-report measures of coping strategies, like those used in this study, can be limited by response biases and may oversimplify the complexity of coping mechanisms, potentially affecting the accuracy of observed patterns [72].
Our previous findings highlighted low self-esteem and low self-confidence in individuals with TXS [17]. Given the relationship between self-esteem and personality—where low self-esteem has been associated with higher neuroticism and lower scores in extraversion, openness to experience, agreeableness, and conscientiousness [73]—and the heritability of both traits (with approximately 30% of the variance attributed to genetic factors; [74,75,76]), we hypothesized that women with TXS would exhibit this personality profile. Contrary to this expectation, no significant differences in personality traits were found between groups. Notably, self-esteem was not assessed in this study, so it remains unclear whether the results of our previous study regarding self-esteem would have been corroborated in our sample.
A central limitation of this study lies in the use of self-report measures, which may be subject to biases such as social desirability or inaccurate self-perception. This is particularly relevant when assessing sensitive topics such as social anxiety, coping strategies, and emotion regulation. Additionally, while the study carefully matched groups based on age and education, other potentially important socio-economic factors, such as employment status, income, and housing conditions, were not systematically assessed. These factors could significantly influence the psychological well-being and social challenges of the participants and should be more thoroughly considered in future studies. Moreover, comorbid conditions, such as ADHD, were not assessed in this study, despite the higher prevalence of ADHD in individuals with TXS [2, 22], which could potentially affect cognitive and emotional outcomes. The cross-sectional design of the study also limits the ability to draw causal conclusions about the relationship between TXS and the observed psychological and social phenomena. Longitudinal studies would provide valuable insights into how these traits evolve over time. Additionally, the recruitment of participants primarily from a self-help group may introduce a bias toward individuals who experience more pronounced symptoms, as those with fewer challenges might be less likely to seek support from such groups. This could lead to an overrepresentation of more severe cases in the sample, skewing the results. At the same time, participation in a study requires a certain level of willingness, courage, and commitment. Therefore, it is conceivable that women with TXS who are more severely affected may not have been willing or able to fill out extensive questionnaires and, as a result, were not included in the study. In this context, findings from the large Danish iPSYCH2015 case-cohort study [2] are particularly relevant: the study found that all examined sex chromosome aneuploidy (SCA) karyotypes (X, XXX, XXY, XYY) were linked to an increased risk of psychiatric disorders, which was similarly present in individuals both with and without a clinical SCA diagnosis. This suggests that psychiatric vulnerabilities in TXS and other SCAs occur independently of clinical detection and similarly affect undiagnosed populations. Lastly, the education matching process itself could introduce a bias, as participants in the control group who were matched for education might come from specific socio-economic backgrounds, which could influence their responses and outcomes. Notably, women with TXS are associated with a lower socio-economic status [71], which typically correlates with lower educational attainment. As a result, the control group participants, who were matched based on education, may have below-average educational levels and therefore may not fully represent the general population. This could explain why the control group often exhibited higher scores compared to normative data, potentially distorting the comparison. Moreover, since education can act as a proxy for cognitive ability, matching on this variable may inadvertently mask true group differences, highlighting a methodological trade-off between controlling confounds and potentially underestimating effects.


Comments (0)