In this investigation, we uncovered a hidden prolonged outbreak involving the high-risk clone P. aeruginosa ST111 blaVIM−2 in a hospital in northern Germany, which had not been recognised as an outbreak by routine epidemiological surveillance. A purely epidemiological assessment was hindered by its prolonged nature over five years going along with patient transfers, external stays, and re-admissions with colonization or infection possibly being misclassified as externally acquired. Hence, epidemiological assessment alone carries the risk to detect only a fraction of the actual transmissions. The frequent occurrence of P. aeruginosa ST111 blaVIM−2 isolates, defined as highly related cluster in molecular surveillance, prompted a closer examination of its epidemiology. From an epidemiological perspective, patient-to-patient transmission was ruled out as there was no direct contact between these patients, all of whom had been hospitalised in ward A but during different periods of time. The investigation of further common procedures like dialyses and bronchoscopy were also excluded, as not every aforementioned patient was dialysed or got a bronchoscopy, especially prior to infection with P. aeruginosa ST111 blaVIM−2. However, all patients were associated with a stay in two adjacent patient rooms in ward A. As a result of this retrospective epidemiological analysis, repetitive environmental sampling was performed on ward A.
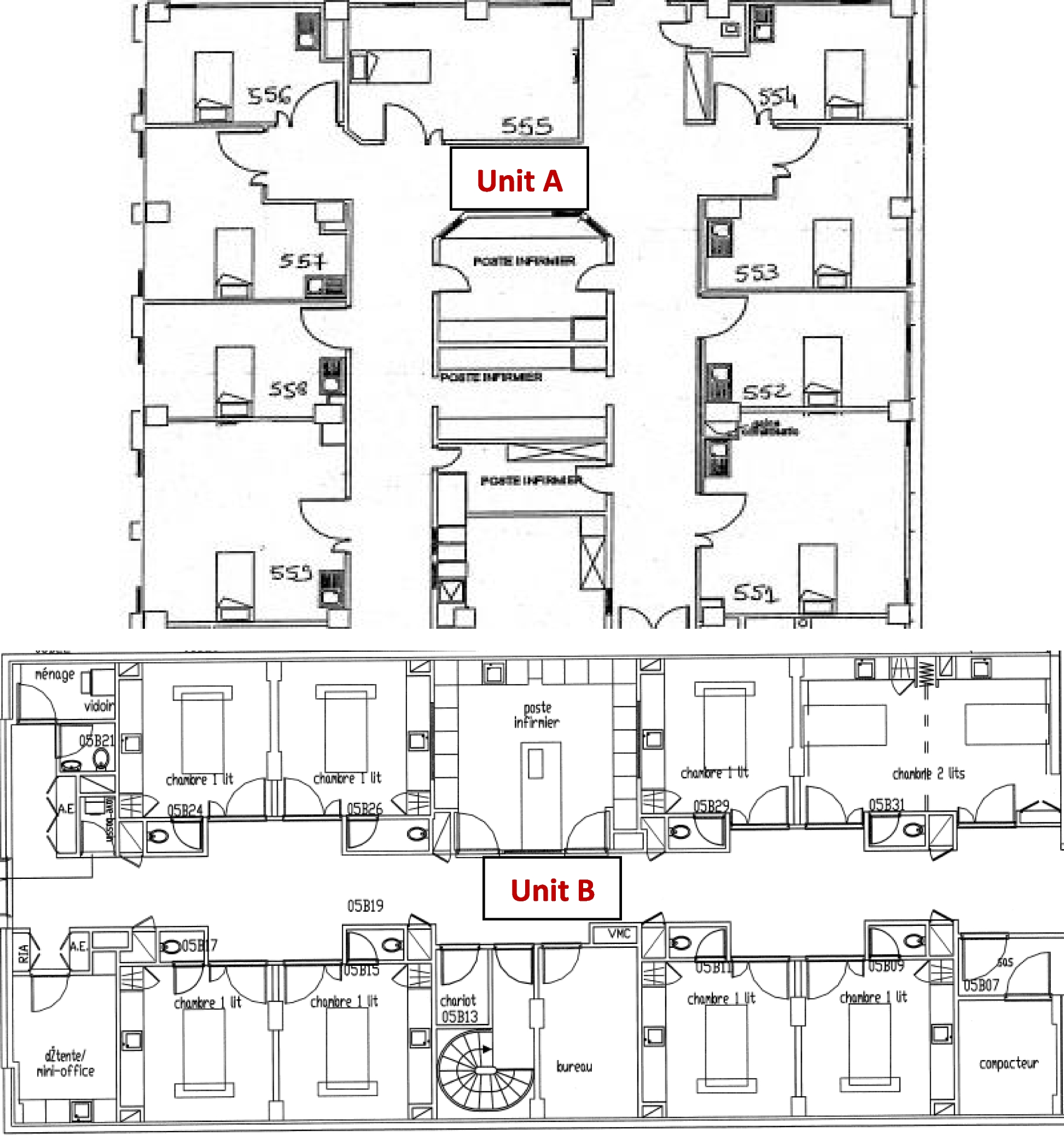
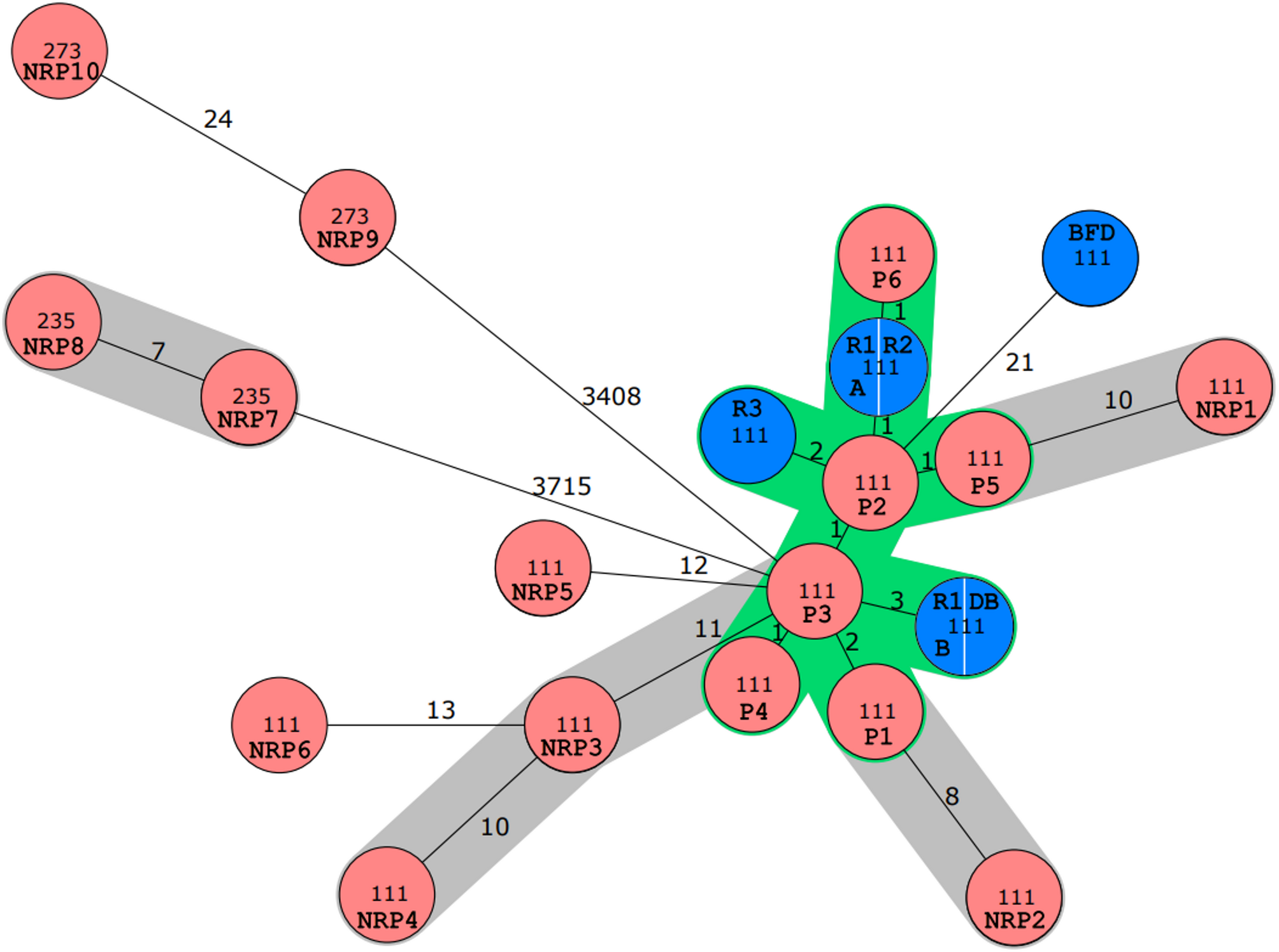
The observation of allelic differences far less than the distance threshold for genomic relatedness of ≤ 11 different in five environmental and clinical isolates of P. aeruginosa ST111 blaVIM−2 proved a nearly identical clone and confirmed sink-to-patient transmission for these cases [14, 15]. Indeed, sink colonisation by MDR Gram-negative bacteria is well documented and is considered as a potential transmission route, frequently associated with HAIs and posing a risk even in non-outbreak situations [16, 17]. Efforts to replace or eradicate contaminated sinks have been employed, but often fail [18], and it is even recommended that ICU rooms should not be equipped with sinks [19]. Our findings align with this, as the environmental P. aeruginosa ST111 blaVIM−2 strain remained detectable in 2023, despite its initial molecular detection occurring four years earlier. However, only six P. aeruginosa ST111 blaVIM−2 infections were traced back to specific sinks in the ICU, though it is assumed that ST111 persists throughout the year in patients [20]. If the infections with ST111 were indeed hospital-acquired, the initial classification of some cases as ‘externally acquired’ under the KISS definition would no longer apply. However, the environmental samplings showed ten different P. aeruginosa ST111 blaVIM−2 isolates indicating the overall frequency of sink-to-patient transmission was low but increased with the length of hospital stay as R1 and R2 was often occupied by patients with long-term stays, while patients in R3 did not. However, Rath et al. analysed the toilet-to-patient transmission rate of ST235 blaFIM−1 and ST309 non-carbapenemase producing P. aeruginosa in a bone marrow transplant unit with cgMLST, showing only a low-genetic diversity but only three toilet-to-patient-transmission over six years [21]. Indeed, our reported ward was originally built as an intermediate care unit and was converted into an intensive care unit later on. As a result, the washbasins were not located directly in the patient’s room but in a separate bathroom, which might have reduced the frequency of transmission.
In addition, alternative transmission routes must be considered. The positive screening of a dialysis therapy bag, placed above the washbasin suggests a possible transmission route, though not all patients were receiving dialysis. Rather, the dialysis therapy bag may represent a potential sink-to- environment-transmission, which might have been favoured by different pressure conditions leading to sink-to-environment-transmission. Bronchoscopy was excluded as a common transmission route as well as other environmental sources on epidemiological basis. However, it should be noted that environmental investigation was initiated four years after the first detection of P. aeruginosa ST111 blaVIM−2 and hence, potential transmission routes might have been missed meanwhile.
Interestingly, the first P. aeruginosa ST111 blaVIM−2 isolate was already detected in 2019 in a patient in screening and blood culture, which was conducted on admission to ward A and was declared as externally acquired since the patient was transferred from an external hospital where the patient was treated for one month. Before that, the patient had hospital stays in our hospital, but remained on normal wards. A P. aeruginosa was never detected. All other cases in the cluster occurred after the admission of the index case bringing up the discussion that first the outbreak stem was transmitted from patient to sink following hidden sink-to-patient transmission and leading to the hidden outbreak. We found a median duration of 20 days from admission to infection with the outbreak strain, which is lower than reported by Volling et al. [22]. However, Volling et al. reported a non-ST111 P. aeruginosa outbreak strain. In the two externally acquired cases colonisation time a maximum of 298 days and 130 days, respectively, is suggested. Notably, during this period both patients were not continuously hospitalized, making it hard to estimate the colonization-to-infection-period.
In our study, the qacEΔ1 resistance gene was detected in ST111 isolates as part of the In59-type integron, similar to the findings of Rath et al. However, it remains unclear whether this gene contributes to resistance against QAC-based disinfectants or plays a role in outbreak promotion even if a QAC-based disinfectant was used in routine hospital disinfection.
ST111 as well as other ST’s multi-resistance is well-documented, but association to resistance gene qacE∆1 has not been reported so far. Hence, further research is needed to elucidate any direct connections between this clone and qacEΔ1.
The observation of P. aeruginosa ST111 blaVIM−2 isolates with confirmed sink-to-patient transmission in an ICU-setting highlights the vulnerability of ICU patients and the conducive environment for antibiotic selection pressure. Previous studies have similarly documented the predominance of ST111 in ICUs and other high-risk wards, including in Germany, where ST111 blaVIM−2 was identified in a cluster of 15 isolates as well as in a Greek hospital [14, 21, 23]. ST111 strains are frequently associated with carbapenemase production, particularly blaVIM−2, leading to multidrug resistance [24, 25]. By chance, the transmission series might be interrupted by eliminating of the clone from the ward during a reconstruction project.
Limitations
This study has several limitations. First, environmental sampling was conducted four years after the first detection of the high-risk clone in clinical isolates. As a result, earlier environmental isolates and sources may have been missed, limiting our ability to accurately determine the duration of the high-risk clone’s presence in the hospital environment in- and outside the sink. To address this, we propose regular environmental sampling to allow for the timely identification of high-risk clones.
Second, while all patients included in the study were infected with the high-risk clone, only two out of six patients were initially screened for colonisation. Therefore, it is unclear whether transmission of the high-risk clone frequently leads to direct infection or if infection regularly resulted from previously undetected colonisation. Hence, we suggested that long-term patients should be screened during their ICU stay. However, further investigation is needed to determine the required time from colonisation to infection, as well as the trigger factors transforming a colonisation into an infection.
Third, during de novo assembly, blaVIM−2 was located in a chromosomally integrated In59-like integron in some strains. In strains without detectable integration into In59, it is unclear whether this is an artefact of the assembly or whether genetic events have actually taken place. However, the three resistance genes blaVIM−2, qacEΔ1 and sul1 were detected in all ST111 strains. Current literature as well as our detailed analysis of the resistance gene profile does not provide sufficient data directly linking qacEΔ1 to ST111 P. aeruginosa and the role in hospital transmission and infection. Further research is required to elucidate these questions.
Fourthly, the outbreak took place during the pandemic, which led to a change in the usual patient clientele.

Comments (0)