
Remember me
From January 2018 to June 2024, 32 patients were colonized or identified with at least one PA-VIM positive clinical sample: 4 were positive on admission (imported cases were transferred from other hospitals) and 28 acquired PA-VIM in the SICU (Fig. 2). During the study period, the median PA-VIM acquisition incidence was 0.83 (Interquartile range (IQR): 0–1.77) per 1000 PD. PA-VIM acquisition incidence per 1000 PD increased in SICU from 2020. Notably, PA-VIM increased from 0.78 in second trimester of 2018 to 3.86 in first trimester of 2020. Two incidence peaks were observed in the third trimesters 2022 and 2023 (3.15 and 5.24 per 1000 PD, respectively) (Fig. 2).
Fig. 2
Epidemic curve of VIM-producing Pseudomonas aeruginosa (PA-VIM) cases in the surgical intensive care unit (SICU). Surgical Intensive Care Unit (SICU), VIM-producing Pseudomonas aeruginosa (PA-VIM)
Demographics and clinical characteristics of the 32 patients are summarized in Table 1. The median age was 65.0 years (IQR: 59.5–69.0) and sex ratio (M/F) was 1.9. Twenty (62.5%) patients had at least one PA-VIM positive clinical sample and 12 (37.5%) were colonized. The median SICU length of stay was 42 days (IQR: 28.5—79.5). For the 28 (87.5%) patients who acquired PA-VIM during their SICU stay, the median time between SICU admission and PA-VIM acquisition was 25.5 days (IQR: 13.0–37.3). Thirteen (40.6%) patients died.
Table 1 Clinical characteristics of 32 patients with VIM-producing Pseudomonas aeruginosa (PA-VIM)Matched case–control studyA total of 17 cases were matched with 32 controls. Two cases could only be matched to a single control. Factors significantly associated with PA-VIM acquisition in the conditional univariate analysis included exposure to antibiotics and antifungals, the use of a nasogastric tube and enteral nutrition (Table 2 ). In the conditional multivariate analysis including diabetes and enteral nutrition, diabetes was associated with an increased risk of PA-VIM acquisition (OR = 8.78; 95% CI: 0.93–83.1; p = 0.06) as well as enteral nutrition (OR = 4.13; 95% CI: 0.98–17.4; p = 0.05), though not significantly.
Table 2 Factors associated with VIM-producing Pseudomonas aeruginosa (PA-VIM) acquisition determined by a matched case–control studyFollowing the results of this matched case–control study, a review of practices indicated that specific practices were inadequate such as disposal of patients’ body fluids and patient nutrition items in sinks or keeping the same enteral syringe near the sink during the whole patient’s stay.
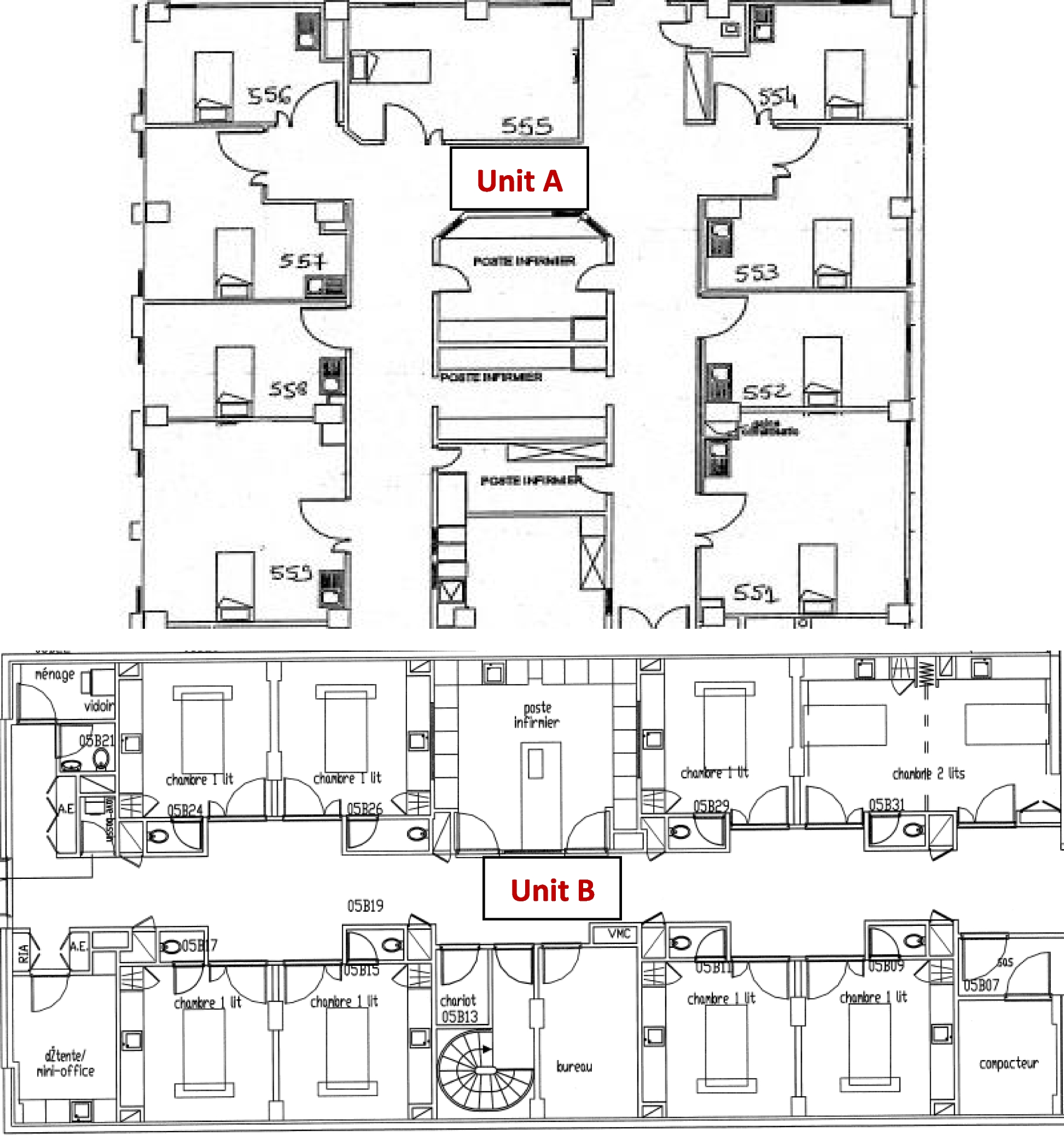
Environmental investigationsBetween February 2020 and June 2024, 342 environmental samples (sink drains, enteral nutrition syringes and glasses where the syringes were placed) were analysed to assess the PA-VIM contamination rate. The overall positivity rate was 19.6% (25.3% for the unit A versus 13.1% for the unit B, p = 0.006) (Table 3). We observed: i) sink drains can be positive independently of patient positivity (e.g., room 557), ii) the drain contamination is often intermittent (e.g., room 551) iii) after the sink drains replacement in February 2020, drain samples remained negative for 9 months, iv) following the matched case–control study, syringes and the glasses were sampled: 2/19 (10.5%) syringes and 2/20 (10.0%) glasses were PA-VIM-positive. A comprehensive figure representing the environmental and patient’s samples positivity over time is described in the additional Figure (see Additional file 1).
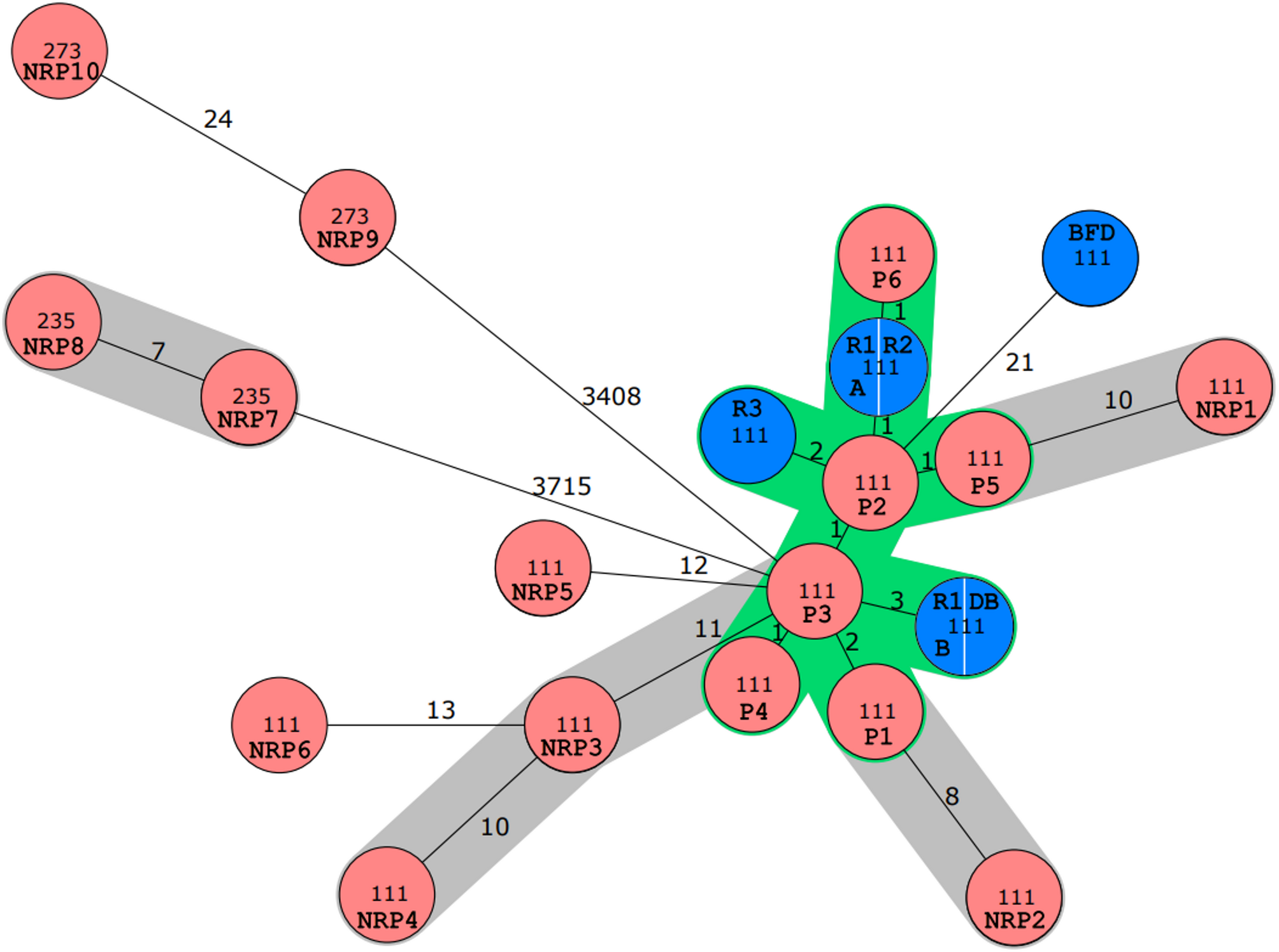
Table 3 Positive environmental samples with VIM-producing Pseudomonas aeruginosa (PA-VIM) in surgical intensive care unit (SICU)Sequencing resultsAmong the isolates collected, 73 were successfully sequenced: 32 samples from 22 patients and 41 from environmental samples. Overall, 2 ST were predominant: ST357 (n = 42, 57.5%) and ST298 (n = 14, 19.2%). Other ST included ST823 (n = 1, 1.4%), ST235 (n = 1, 1.4%) and undetermined ST (n = 15, 20.5%). The blaVIM-2 gene was found as predominant (n = 65, 89%) followed by the blaVIM-4 (n = 8, 11%). Based on the 14 alleles difference threshold, five clusters were identified (Fig. 3).
Fig. 3
Genomic distance of VIM-producing Pseudomonas aeruginosa (PA-VIM) strains by pairwise comparison of core-genes allelic profiles
Each VIM-producing Pseudomonas aeruginosa (PA-VIM) strain is represented by a circle. Each sequence type (ST) is represented by a colour (dark blue: ST357; light blue: undetermined ST; orange: ST298; dark green: ST235; light green: ST823). Each cluster (based on the 14 alleles difference threshold) is represented by a rectangle. Genomes with an allelic distance of zero are aggregated into a single, larger circle. The size of the circle is directly proportional to the number of aggregated genomes. The allelic distance between two strains is represented by a line with a number. A full line means that the allelic distance < 50, while a dotted line means that the distance > 100
The cluster A included 42 isolates of ST357, 19 from patients (14 in unit A from 2020 to 2023 and 5 in unit B from 2022 to 2023) and 23 from environmental samples (18 in unit A from 2020 to 2024 and 5 in unit B in 2023). More specifically, strains from patients 9, 13, 15, 18 and 29 who stayed in room 551 belonged to this cluster and had minimal allelic differences (≤ 6) whatever the date of isolation.
The cluster B included 14 isolates of ST298, 6 from patients from 2022 to 2023 and 8 from environmental samples from 2022 to 2024, only in unit A. More specifically, patients 16, 19 and 26 who stayed in room 555 where the drain, glass and syringe turned out to be positive on 2023–09, belonged to this cluster.
The cluster C included 3 isolates of undetermined ST, from patients in unit B in 2023. The cluster D included 3 isolates of undetermined ST, 2 from patients (one in each unit) in 2019 and 2020 and 1 from an environmental sample in unit B in 2020. The cluster E included 2 isolates of undetermined ST, from environmental samples in unit B (same room) in 2020.
In some cases, there was a clear link between the isolates identified in patients and the contamination of the sink drains. For example, patient 20 was hospitalized from 2022–08 to 2022–09 in room 558 (unit A) in which the sink drain was contaminated with PA-VIM ST357 (positive results on 2022–08 and 2022–09); this patient was then transferred to room 566 (unit B) and the sink drain in room 566 became positive for PA-VIM ST357 on 2024–03.
Patients 21, 23, 25, 26, 29, and 32 acquired PA-VIM following multiple negative screening swabs, during their hospitalization in rooms where sink drains were previously identified as PA-VIM-positive.
Outbreaks control measuresDetection of PA-VIM prompted enhanced infection control procedures which were maintained until patient’s death or discharge. These measures included a tag in the electronic health record, implementation of contact precautions, SICU regular staff education by the Prevention and Control Infection unit members, reminders of standard precautions, sink drains descaling with white vinegar and disinfection with 200 mL of 0.5% hypochlorite.
Before February 2020, a 0.5% chlorine treatment of sinks was performed only upon discharge of each PA-VIM-positive patient. From February to September 2020, a daily disinfection with 0.5% hypochlorite was implemented throughout the ward, irrespective of the patient's status; then as of September 2020 onwards, a weekly hypochlorite treatment was performed throughout the ward. Since September 2022, a weekly descaling of all drains with white vinegar treatment has been added. From September 2023, the syringes used for enteral nutrition and the glasses containing them were replaced by single-use devices. In addition, in February 2020 and June 2024, all SICU drains were replaced (Fig. 2).
Comments (0)