
Remember me
Seven surgeons (three female, four male) with RAS experience participated in 30-min, semi-structured interviews conducted between January and February 2024. The majority (71.4%, 5/7) had learned how to operate on a RAS platform during residency or fellowship training. Two of the interviewed surgeons (28.6%) were not SAGES members.
Based on the themes highlighted below, surgeons felt RAS outperformed LS in three operational areas:
(1) Device Performance—Surgeons perceived that RAS outperformed LS in accuracy, precision, accessibility, and movement. However, the lack of tactile feedback was a notable limitation. As one surgeon remarked:
“For accuracy and precision, I think the robot is better (than laparoscopy)… having the articulated approach does allow you to get into a little bit more precise places…I do think (lack of tactile feedback) that’s a concern with the robot, but I think it’s one that you can overcome by using visual cues to understand tension and tissue motion…” (interviewee FS1)
(2) Intraoperative Teaching—The dual console of RAS systems facilitated easier teaching and skill transfer compared to LS. One participant stated:
“I think the robot is definitely better for (intraoperative) teaching (than laparoscopy). You’re just able to pass it back and forth (between a resident) a lot easier when you have a (robotic surgical system with) dual console.” (interviewee FS2)
(3) Physical and/or Visual Fatigue—RAS was associated with reduced physical and/or visual fatigue compared to LS. For example, one surgeon explained:
“If I did a difficult laparoscopic lithotomy, I would sit between the (patient) legs. I’d be doing this: looking up, trying to sew, straight sticks…If I did it with robot, I would be sitting at the console, much less fatiguing for me… I still get tired just because of the mental strain for the other cases, but I’m much less (physical) fatiguing.” (interviewee MS1)
However, when compared to LS, surgeons also noted three main drawbacks of RAS:
(1) Resource Intensive—RAS usually required a larger operating room (OR) and a proficient team who was familiar with RAS in order to set up the OR and progress through the case efficiently. Additionally, given the cost of the robotic system, most hospitals have not yet been able to install a robotic system in each OR, leading to difficulty in scheduling RAS cases. Furthermore, insurance reimbursement also sometimes contributed to barriers to RAS case scheduling. One surgeon noted:
“The (operating) room is a problem… you need a (operating) room, you need the robot, and you need staff who can take care of that… because the robot is only in a certain room, I have to request it well in advance to find open time… It can be pretty challenging and cumbersome to get access to the robot in this setting.” (interviewee, MS2)
(2) Mechanical Malfunction—Compared to LS, concern about mechanical malfunction of the robotic platform intraoperatively was raised. Surgeons felt that they did not have sufficient knowledge and experience to troubleshoot mechanical dysfunctions, leading to a disruption of the RAS operative workflow (e.g., conversion of RAS to LS or Open). As one surgeon commented:
“The problem with the robotic malfunction is I don’t know what’s going wrong. If a stapler or an instrument fails (in laparoscopy), I know how to fix that… (in terms of robotic malfunction) I just reset the robot and cross my fingers and hope (it would be fixed) ... The biggest issue is I don’t know what’s gone wrong (with the robot). So, if we still cannot fix it, just need to convert it to an open (case).” (interviewee MS3)
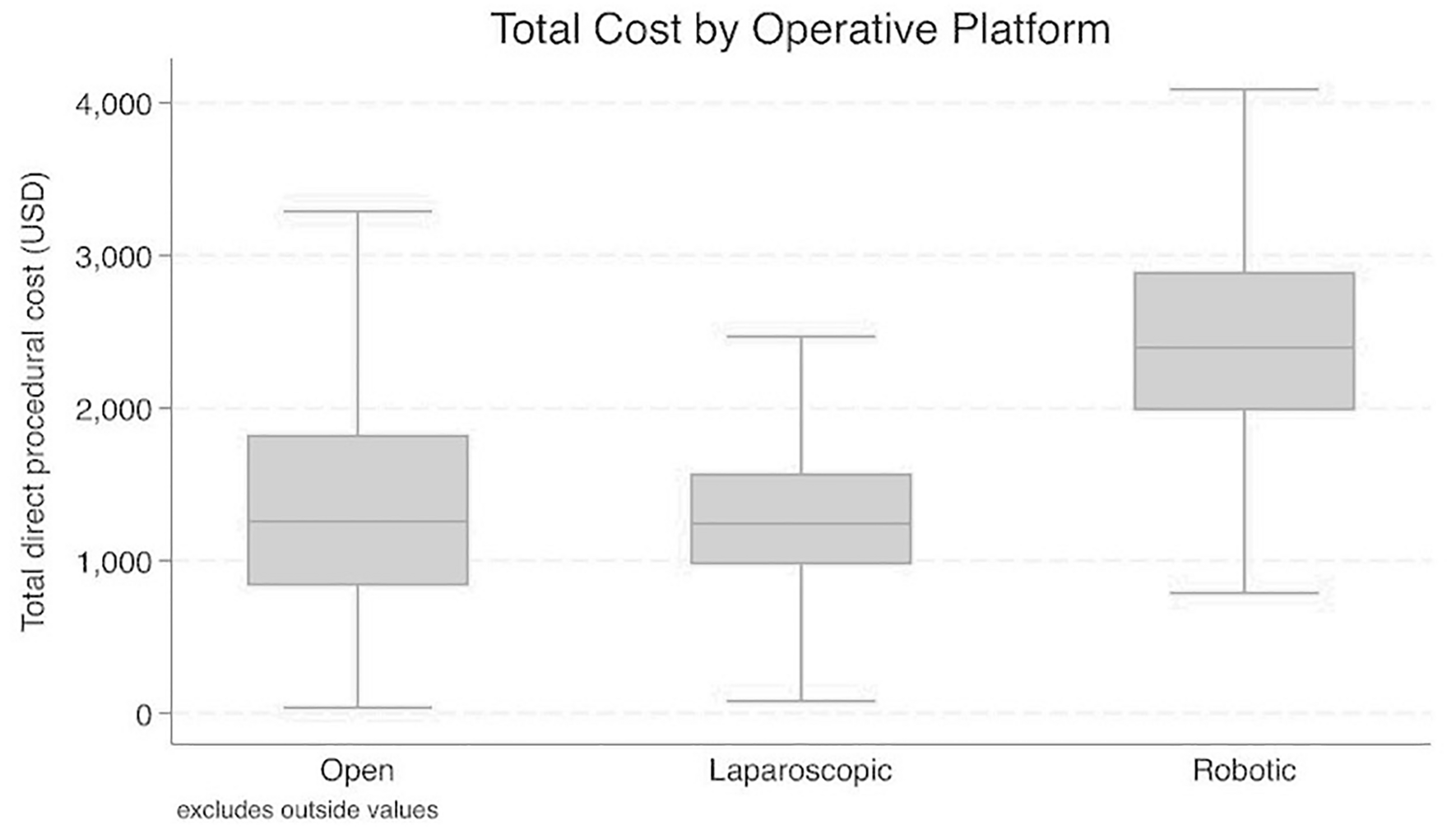
(3) Higher Care Delivery Cost—This included cost of usage as well as reimbursement. For example, a laparoscopic colectomy and a robotic colectomy use the same Current Procedural Terminology (CPT) code for billing and reimbursement, but the total costs of performing a robotic colectomy were higher than a laparoscopic colectomy. It was suggested that the surgeons’ experience and knowledge of RAS disposable costs may help to increase cost-efficiency. As one surgeon said:
“I try to be conscientious of what instruments I’m using (in the RAS case) and have knowledge of what the cost of those instruments are. Because if it’s not put in the robot and activated, it doesn’t get charged for that case and I think surgeons should know that.” (interviewee FS1)
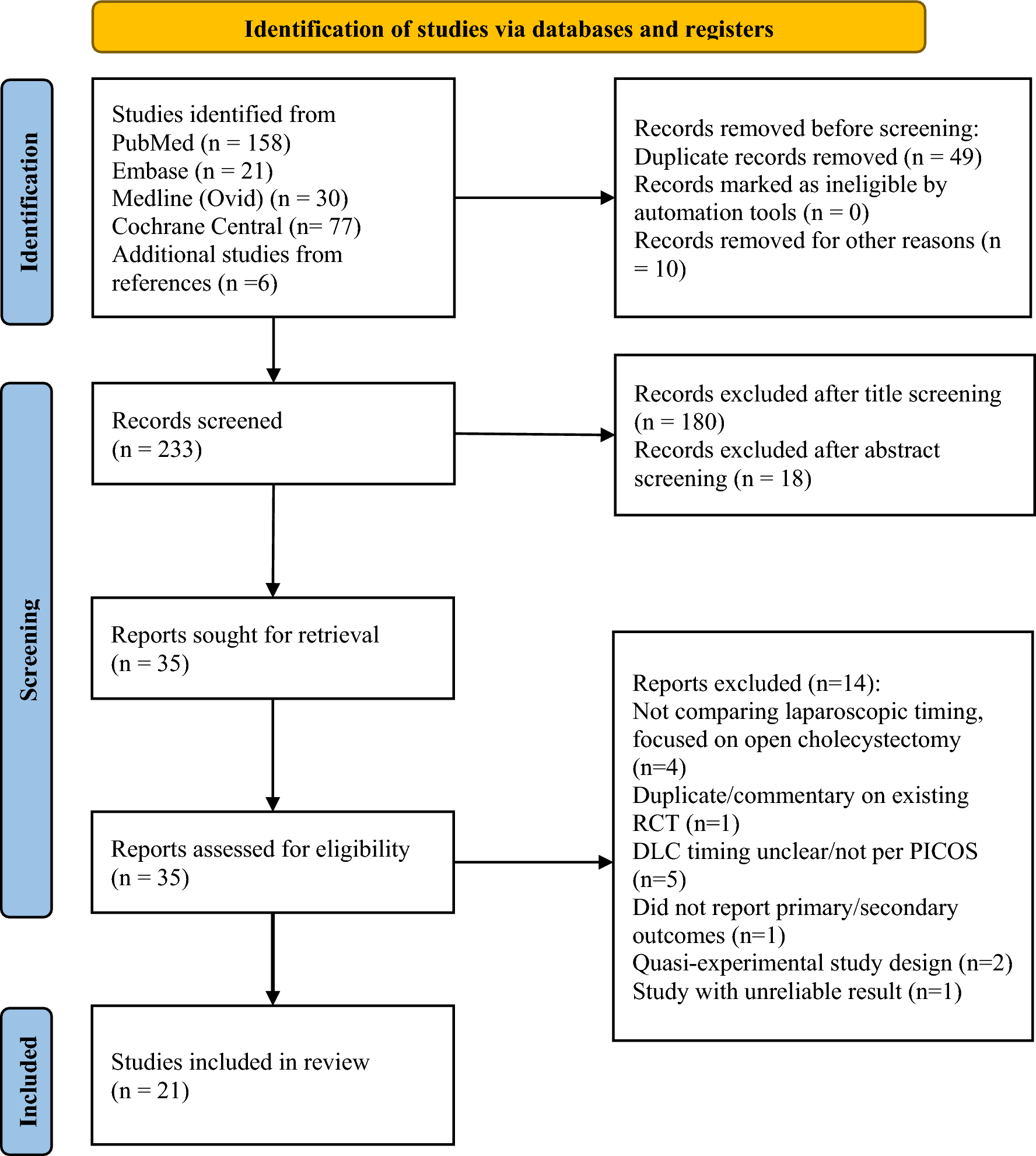
Quantitative surveyA total of 55 SAGES Robotics Committee surgeons (59.8% response rate) completed the survey (Fig. 1). Respondents were male (50.9%, 28/55), practiced in academic settings (80%, 44/55), and had learned RAS during residency or fellowship (70.9%, 39/55). Most participants (63.6%, 35/55) performed over 10 RAS cases per month, with 5.5% (3/55) also having experience using systems other than the da Vinci platform (Intuitive Surgical, Sunnyvale, CA, USA).
Fig. 1
Survey results confirmed interview themes and revealed additional insights (Table 1).
Table 1 Comparison between robotic and laparoscopic surgeryIn the “utilization performance” domain, surgeon participants indicated that when compared to LS, RAS significantly improved the operational performance in three out of six aspects: “Access to Difficult Areas” (3.84 > 2.36, p < 0.001), “Accuracy and Precision” (3.80 > 2.45, p < 0.001), and “Facilitation of OR Teaching” (3.56 > 2.57, p < 0.001). However, RAS significantly underperformed LS in “Tactile Feedback” (1.60 < 3.31, p < 0.001). In general, “Frequency of Mechanical Malfunctions” was reported to be similar between RAS and LS. Female surgeons demonstrated lower satisfaction with the frequency of mechanical malfunctions in RAS than male surgeons (2.48 < 3.07, p = 0.018).
In the “utilization requirements” domain, compared to RAS, LS cases were noted to be significantly easier to schedule (3.20 > 2.27, p < 0.001) and more OR-space-friendly (2.95 > 2.02, p < 0.001). On average, surgeons perceived that “Malfunction troubleshooting tech support” was similar between RAS and LS, but female surgeons indicated insufficient technical support for troubleshooting robotic surgical system mechanical malfunctions specifically (2.19 < 2.82, p = 0.017).
In the “utilization challenges” domain, surgeons reported perceiving an easier learning curve for RAS than LS (3.31 > 2.07, p < 0.001). Whether a surgeon had learned RAS during residency or fellowship training had no impact on their perceived RAS learning curve score (3.31 vs. 3.31). Surgeons also reported feeling that it was significantly easier and more convenient to grant a trainee autonomy in RAS than in LS. Compared to LS, surgeons indicated Do-It-Yourself (DIY) troubleshooting mechanical malfunctions in RAS was more difficult.
In the “utilization care outcomes” domain, surgeons perceived that RAS significantly outperformed LS in two aspects: “Intraoperative Complications” (3.65 > 3.18, p = 0.0002) and “Blood Loss” (3.67 > 3.09, p < 0.001). LS had a perceived superior performance in “Total Patient Care Delivery Cost” (3.11 > 2.22, p < 0.001) compared to RAS. In terms of the “Length of Procedure,” male surgeons perceived RAS as having better time-efficiency outcomes than female surgeons (3.18 > 2.59, p = 0.022), but reported similar scores for LS (2.75 vs 2.78).
We also asked surgeon participants to rank their desired extra RAS functions that could be added on in future, as well as to grade the helpfulness of support needed from and provided by SAGES (Table 2). Among the four options, 36.4% (20/55) surgeons ranked “Artificial Intelligence (AI)-assisted Navigation/Guidance” as the “most wanted” new RAS add-on function while 30.9% (17/55) selected it as the “least wanted” new RAS function. The second “most wanted” new RAS function was “Flexible Ergonomic Design” (30.9%, 17/55), followed by “Error Movement/Malfunction Warning System” (21.8%, 12/55). Regarding the support needed from SAGES, the three highest ranked support items were as follows: “Develop Robotic Surgery Skills Curricula for Trainees and Practicing Surgeons” (3.56 ± 0.57), “Develop Best Practice Guidelines for Robotic Surgery” (3.44 ± 0.81), and “Develop Tools for Robotic Surgery Performance Assessment” (3.42 ± 0.76).
Table 2 List of desired additional robotic functions and SAGES Help/support
Comments (0)