Surgeon practice patterns drive procedural cost variation in appendectomy without improving short-term outcomes
Background
Appendectomy is a common emergency general surgery procedure and is now performed predominantly using minimally invasive techniques. While robotic platforms have diffused in elective general surgery, their role in appendectomy remains limited. Surgeon-level cost variation in emergency general surgery is not well defined.
Methods
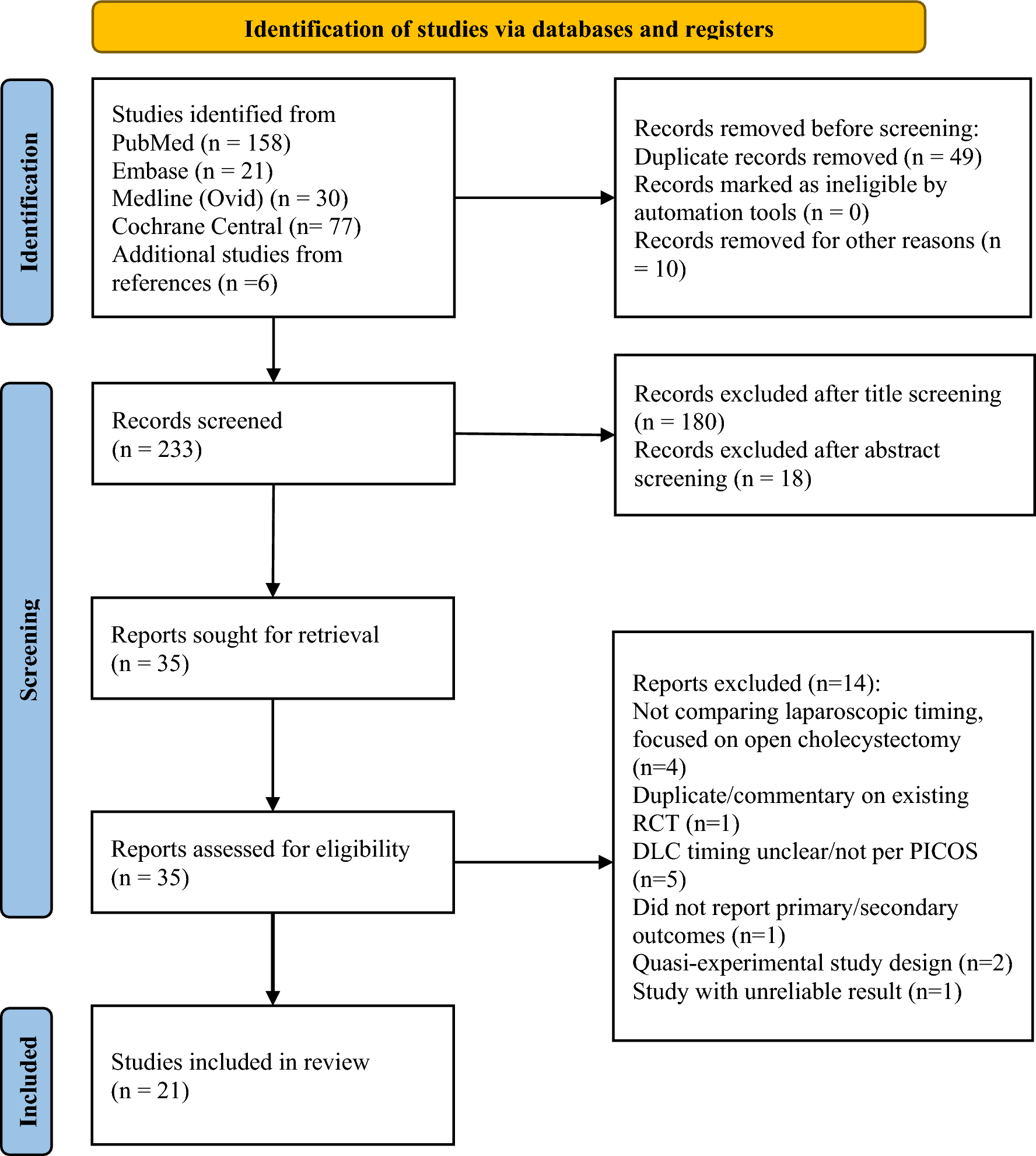
We performed a retrospective cohort study of adult patients undergoing appendectomy across a large integrated healthcare system from 2017 to 2025. Operative approach was categorized as open, laparoscopic, or robotic. The primary outcome was total direct procedural cost. Secondary outcomes included operating room (OR) time, postoperative length of stay (LOS), and 30-day reintervention. Hierarchical mixed-effects regression models with surgeons nested within hospitals were used to evaluate associations between operative approach, provider-level effects, cost, and outcomes.
Results
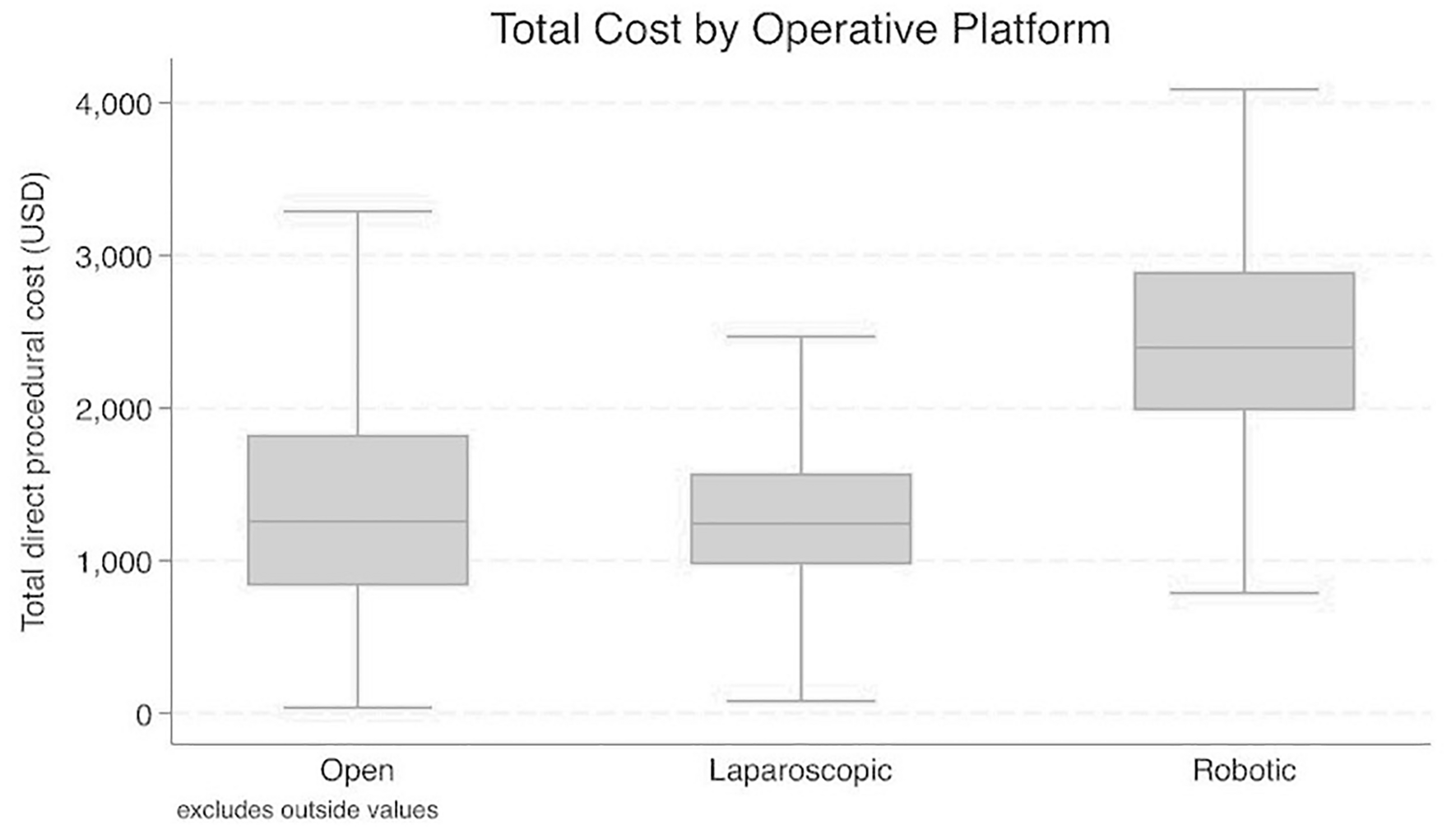
The cohort included 11,153 patients treated by 286 surgeons across 26 hospitals. Laparoscopic appendectomy accounted for 95.3% of cases, robotic for 2.4%, and open for 2.3%. Substantial procedural cost variation persisted after adjustment. Surgeon-level effects accounted for approximately 28% of residual cost variation, compared with 11% attributable to hospitals, with an interdecile range of adjusted surgeon-specific cost effects exceeding $400 per case. Robotic appendectomy was independently associated with higher procedural cost but remained infrequently utilized. Higher operative cost was associated with longer OR time and longer LOS, without improvement in short-term outcomes. Thirty-day reintervention was uncommon (0.84%) and was independently associated with operative approach and patient acuity, but not with higher spending or provider-level effects.
Conclusions
In appendectomy, surgeon practice patterns are a dominant driver of procedural cost variation, while higher spending does not confer improvements in efficiency or short-term clinical outcomes. These findings demonstrate a disconnect between cost and value in emergency general surgery and identify surgeon-focused cost transparency and selective standardization as practical, actionable strategies to improve value without compromising patient safety.

Comments (0)