
Remember me
Robotic liver resection was started at our institution in June 2022. After an initial implementation period, the surgeon-controlled robotic CUSA technique was adopted as the standard method for parenchymal transection. The initial 4-month period was excluded to allow for team maturation and the stabilization of the robotic operative workflow before outcome assessment. Surgical outcomes were evaluated using a prospectively maintained institutional database. In this retrospective study, we analyzed consecutive patients with preserved hepatic function (Child–Pugh class A) who underwent robotic liver resection without additional concomitant procedures, performed by the same surgical team to minimize procedural variability. The primary outcome was the incidence of at least Clavien–Dindo grade IIIa postoperative complications. Secondary outcomes included parenchymal transection time, estimated blood loss, and resection margin status.
Informed consent was obtained from all patients in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of the International University of Health and Welfare (approval number: 21-Nr-008).
PatientsBetween October 2022 and December 2025, consecutive patients who underwent robotic liver resection at our institution were retrospectively reviewed. During the early period, parenchymal transection was performed using the clamp-crush technique. After a transition phase, the surgeon-controlled CUSA method became the standard approach in the later period. All procedures were performed by two board-certified expert hepatobiliary surgeons (TM and OI) accredited by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. Robotic platforms included the da Vinci Xi system and the hinotori Surgical Robot.
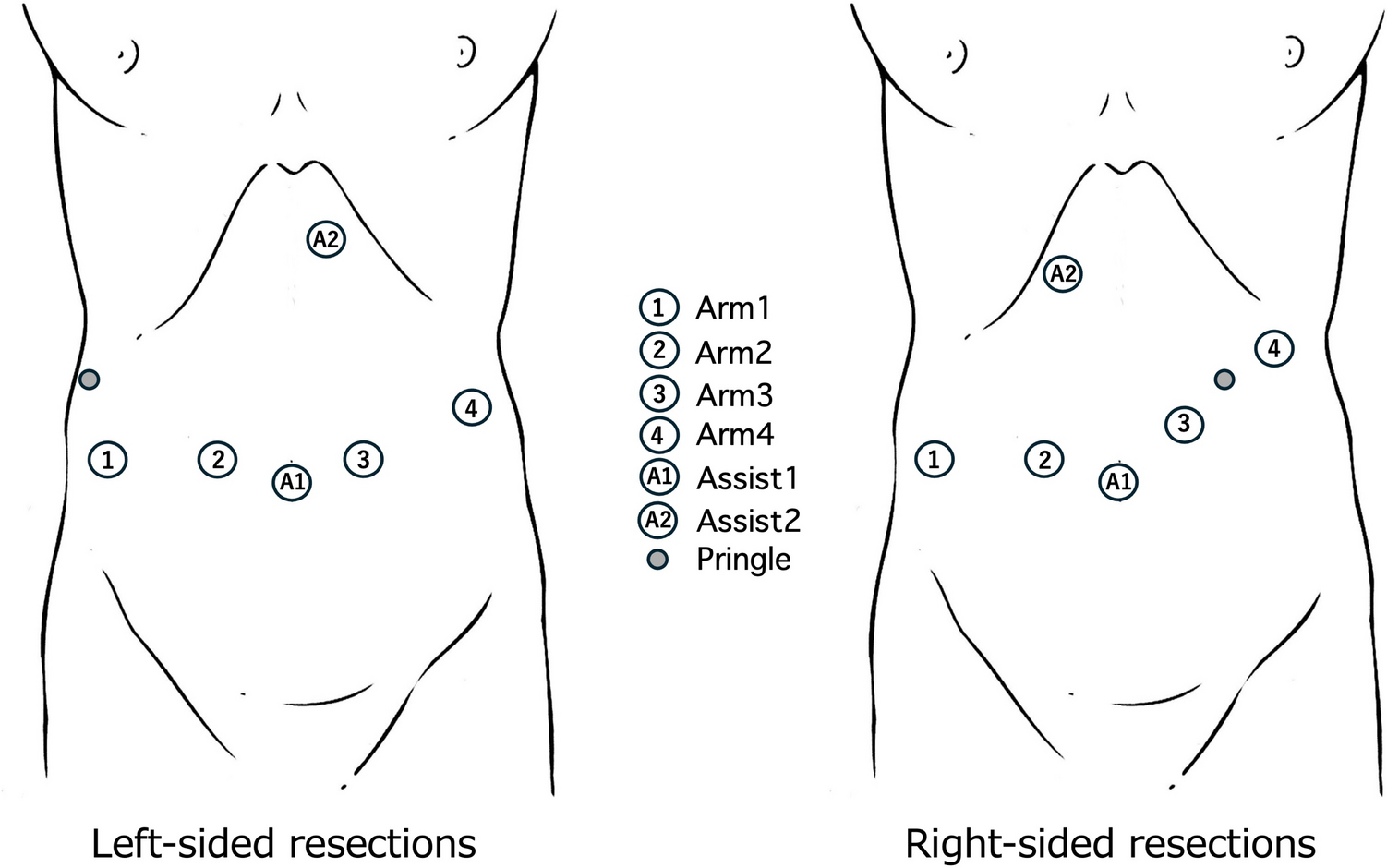
Surgical techniquePort placementThe port configuration was adjusted according to the tumor location. For left-sided resection, the robotic trocars were aligned horizontally. For right-sided resections, arms 3 and 4 were positioned slightly cranially to optimize access to the hepatic hilum and posterosuperior segments (Fig. 1). When targeting lesions in Segments 7 and 8, the entire layout was shifted cranially.
Fig.1
Port placement and assistant port selection for robotic CUSA manipulation. Schematic illustration of port placement for the surgeon-controlled robotic CUSA technique. Robotic port configuration is adjusted according to tumor location, with left-sided resections arranged horizontally and right-sided resections positioned more cranially. An additional 12-mm assistant port is placed either caudally or in the epigastric region for CUSA insertion. The caudal assistant port is primarily used for inferior segments (S3, S4b, S5, and S6), whereas the epigastric port is preferred for superior and posterosuperior segments (S2, S4a, S7, and S8), minimizing arm collision and optimizing the transection angle
An additional 12-mm assistant port was required for CUSA insertion. To secure an optimal working angle for the parenchymal transection, the port was placed either slightly caudal to the robotic ports or near the epigastrium. In practice, the caudal assistant port is mainly used for the inferior segments (S3, S4b, S5, and S6), whereas the epigastric port is selected for the superior segments (S2, S4a, S7, and S8).
To prevent collisions with the robotic arm manipulating the CUSA (typically Arm 3), the caudal assistant port should not be placed parallel to it and should be positioned at a sufficient offset distance. The epigastric port offers a more vertical trajectory and is less prone to interference.
CUSA tip attachment modificationA simple handmade attachment was created to enable the robotic manipulation of the CUSA (Video S1). A strip of Tetron tape was tied around the proximal end of the tip of the CUSA and fixed with silk sutures to form a firm gripping zone for the robotic arm. Additional silk sutures and adhesive film tape reinforced the attachment to prevent forward slippage (Fig. 2). This configuration provides adequate stability and safe force transmission.
Fig. 2
Handmade CUSA attachment for robotic manipulation. Step-by-step creation of a handmade attachment for robotic manipulation of the CUSA. Silk sutures are first fixed to the proximal portion of the CUSA tip. A Tetron tape is tied above the silk sutures to create a dedicated gripping zone for the robotic arm. The attachment is reinforced with additional silk ligatures at multiple fixation points to prevent slippage. Excess Tetron tape is secured to the CUSA shaft using adhesive film tape to enhance stability and handling during prolonged parenchymal transection
No structural damage to CUSA devices was observed in our series; however, prolonged procedures may loosen the handmade attachments. Periodic reinforcement or replacement during surgery is recommended to maintain the required stability.
Robotic handling of CUSAThe robotic arm grasped the customized gripping zone, enabling precise control of the CUSA tip direction, angle, and countertraction directly by the console surgeon (Fig. 3). CUSA activation was controlled using a foot switch on the console. This represents a core innovation enabling surgeon-led parenchymal transection in a robotic setting (Videos S2, S3).
Fig. 3
Surgeon-controlled robotic CUSA technique for liver parenchymal transection. Intraoperative views demonstrating the surgeon-controlled robotic CUSA technique for liver parenchymal transection. A The robotic arm directly grasps the customized gripping zone of the CUSA, allowing precise control of the tip direction and angle by the console surgeon. B Parenchymal transection is performed using characteristic CUSA techniques, including boring and shoveling, with stable visualization of fine intrahepatic anatomy. C Safe exposure of Glissonean branches, and D hepatic veins is achieved through controlled cranio-caudal and ventro-dorsal movements under direct robotic control. RHV, right hepatic vein
Vertical CUSA motion is easier robotically, whereas lateral motion tends to be restricted. Therefore, adjusting the transection plane to favor an up-and-down motion improves efficiency. Adequate extracorporeal or intracorporeal traction enhances visualization and force transmission. For posterosuperior lesions (S7 and S8), manipulation is challenging because of the diaphragm and rib cage. Therefore, full liver mobilization is essential to secure a safe approach.
Role of the assistantThe bedside assistant surgeon supports the proximal CUSA shaft extracorporeally and operates the soft-coagulation energy mode using a hand or foot switch (which may be alternatively controlled by the console surgeon). Because the CUSA simultaneously provides suction and hemostasis, the assistant can devote attention mainly to maintaining the operative field and assisting with energy activation as needed without requiring advanced technical skills.
Statistical analysisPatient demographics, liver function, tumor characteristics, operative variables, and postoperative outcomes were compared between the clamp-crush group and the surgeon-controlled CUSA group. Statistical analyses were performed using SPSS software version 28.0 (IBM Corp., Chicago, IL, USA). Continuous variables were compared using the Mann–Whitney U-test, and categorical variables were analyzed using the χ2 test or Fisher’s exact test, as appropriate. A p value < 0.05 was considered statistically significant. Given the limited sample size, non-inferiority testing was not formally performed; comparisons were exploratory and hypothesis-generating.
Comments (0)