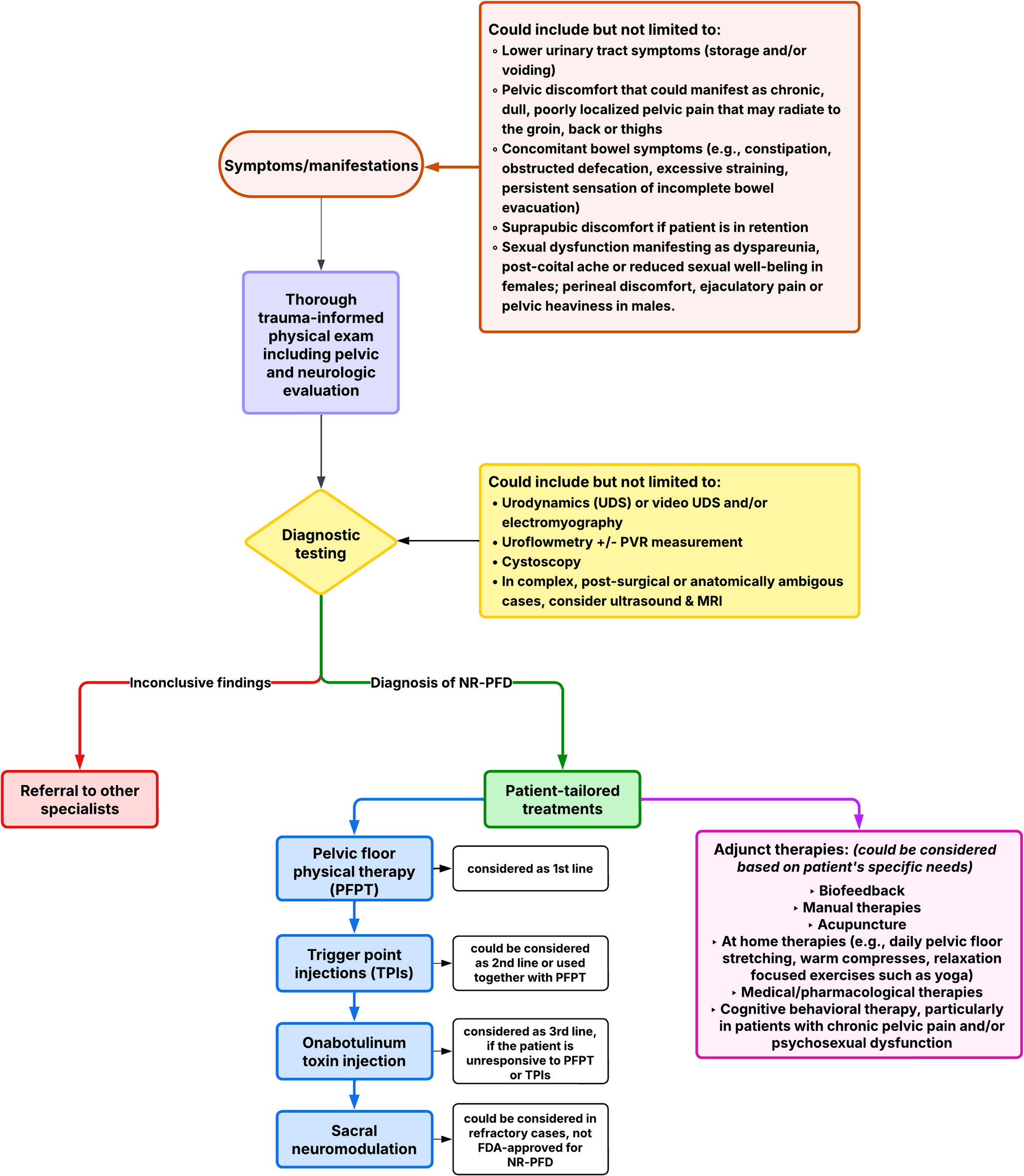
Managing urologic symptoms from NR-PFD is complex and must be tailored to each patient’s unique presentation. Due to the variability in symptoms, especially when pelvic pain and non-urologic issues overlap, a multidisciplinary, multimodal approach is essential. (Table 1) Collaboration among urologists, other specialists (colorectal, gynecology, etc.), pelvic floor physical therapists, pain specialists, and behavioral health providers ensures comprehensive care. Key goals include restoring normal voiding, reducing symptoms, and preventing complications such as UTIs, bladder dysfunction, hydronephrosis, and long-term renal damage.
Table 1 Summary of literature evaluating available treatment modalitiesPelvic Floor Physical Therapy, Biofeedback, and Manual Therapies
Pelvic floor physical therapy (PFPT) is the first-line treatment for NR-PFD and serves as the foundation of conservative management for urologic symptoms related to pelvic floor hypertonicity and/or impaired relaxation [42]. It is most effective when delivered by therapists trained in pelvic floor rehabilitation and incorporates interventions such as neuromuscular re-education, diaphragmatic breathing, core stabilization, and reverse Kegel exercises that enhance pelvic floor coordination and reduce muscle overactivity.
Biofeedback can enhance PFPT by helping patients identify and relax overactive pelvic muscles, especially when symptoms are thought to stem from learned behaviors [43]. In a randomized trial, Minardi et al. found that uroflowmetry-based biofeedback with pelvic muscle training significantly reduced UTIs and improved voiding parameters [44]. For patients with chronic pain, biofeedback may facilitate deeper muscle relaxation. Education on posture, behavioral triggers, and pelvic awareness is also essential [6, 22].
PFPT has demonstrated efficacy across sexes. For men, PFPT has shown to be an effective modality in improving high-tone pelvic floor dysfunction. Polackwich et al. observed that 79% of men achieved clinically meaningful improvement in NIH Chronic Prostatitis Symptom Index (NIH-CPSI) scores, including voiding-related metrics such as urinary frequency, incomplete emptying, sexual dysfunction, and pelvic pain with PFPT [45]. Additionally, biofeedback-assisted PFPT has demonstrated efficacy in reducing pelvic floor tone and symptom burden among men with both chronic pelvic pain and bothersome urinary symptoms [46].
In women, PFPT, when used alone or in combination with biofeedback and relaxation training, has demonstrated similarly high success rates in treating non-relaxing pelvic floor tonicity and lower urinary tract symptoms. In a prospective study, 81% of women achieved clinical and uroflowmetric improvements after 3 months of biofeedback-assisted PFPT [47]. Meta-analyses confirm PFPT as the most effective conservative treatment for urinary incontinence and broader LUTS in women with high-tone pelvic floors, improving symptom severity and urodynamic measures [48, 49]. The RELAX trial (Volpe et al.) demonstrated significant levator hiatal lengthening after six sessions of PFPT, accompanied by improvements in pelvic pain, bowel, bladder, and quality-of-life metrics [16, 50].
Experts in Torosis et al. unanimously endorsed PFPT as first-line therapy for hypertonic pelvic floor dysfunction, recommending 1–2 sessions weekly for 8–12 weeks. Following symptom improvement, patients should be advised to follow a home exercise regimen and undergo follow-up at 4–6 months [42].
Medical/Pharmacological Therapies
Pharmacologic management is considered adjunctive and should be tailored to the patient’s most bothersome symptoms, as most medications do not directly address the underlying neuromuscular dysfunction and are not first-line treatments.
Muscle relaxants, such as oral baclofen, tizanidine, cyclobenzaprine, and diazepam, may reduce pelvic floor spasm and provide symptom relief. Diazepam suppositories are the most commonly prescribed vaginal formulation and are preferred over oral routes due to lower systemic absorption and longer local activity, resulting in fewer side effects [42].
Neuropathic pain agents, including amitriptyline, nortriptyline, gabapentin, and pregabalin, are often used for chronic pelvic pain, though tricyclic antidepressants may exacerbate bowel or bladder symptoms and are generally avoided in NR-PFD [2].
In patients with overlapping overactive bladder symptoms, anticholinergics (e.g., fesoterodine, tolterodine) and β3 agonists (e.g., mirabegron) may modestly improve urgency. However, these agents do not address pelvic floor dysfunction and are ineffective for voiding symptoms related to non-relaxation; their use should be limited to cases where urgency predominates.
Trigger Point Injections
Trigger point injections (TPIs) are considered second-line or adjunctive therapies for NR-PFD, particularly in patients unresponsive to PFPT. A myofascial trigger point is a tender nodule within a taut muscle band, often seen in hypertonic muscles, though not all tight muscles exhibit localized tenderness [22, 51]. As such, TPIs are most appropriate when focal tender points can be reliably identified.
The standard technique involves palpating pelvic floor muscles perpendicular to their fibers to detect taut bands, then along the fibers to find the most symptomatic point. Local anesthetic (typically 0.25–0.5% bupivacaine) is injected into this site. Corticosteroids may be added but offer no proven advantage. Expert consensus favors an anesthetic alone [42].
TPIs do not directly relax muscle tone but may reduce pain and interrupt the guarding reflex, facilitating downstream pelvic floor relaxation. In one study, levator ani TPIs improved symptoms by > 50% in 72% of patients with chronic pelvic pain [52]. In men with urologic chronic pelvic pain syndrome and pelvic floor hypertonicity, ultrasound-guided TPIs to muscles such as the iliococcygeus, pubococcygeus, and hip adductors improved NIH-CPSI and pain scores after a short treatment course [53]. Similarly, in women, TPIs with local anesthetic reduced pelvic myalgia and urinary symptoms (e.g., urgency and frequency) in those refractory to physical therapy [54, 55].
Experts in Torosis et al. reached no consensus on the use of anesthesia during TPIs. Additionally, pudendal nerve blocks are not indicated for NR-PFD unless pudendal neuralgia is suspected or diagnostic clarification is needed; they are ineffective for pure muscle hypertonicity without neuropathic features [42].
Botulinum Toxin A
Botulinum toxin A (BTXA) is considered a third-line option for refractory pelvic floor hypertonicity or myofascial pain unresponsive to PFPT or other conservative therapies. Per expert consensus, BTXA should be injected directly into hypertonic or non-relaxing muscles and used alongside continued PFPT. Injections are typically bilateral, and lack of response after 1–2 sessions should prompt transition to alternative treatments [42].
BTXA may reduce pain via both muscle relaxation and modulation of nociceptive [56]. However, randomized controlled trials in women with pelvic floor hypertonicity and chronic pelvic pain—groups overlapping with NR-PFD—have not shown BTXA to outperform placebo in improving pain, urinary symptoms, or global function, even when combined with PFPT [57, 58]. While minor improvements in resting pressure and quality of life have been reported, they have not translated into significant clinical benefit for urologic outcomes.
There is wide variability in dosing protocols. Reported regimens range from 10 to 50 units per muscle group, depending on the number and location of the targeted muscles. Total BTXA dosing should not exceed 360 units within a three-month period [42]. BTXA use in hypertonic or NR-PFD remains off-label, and further studies are needed to define its role in urologic symptom management.
Sacral Neuromodulation
Sacral neuromodulation (SNM) may be considered for patients with persistent voiding dysfunction or pelvic pain unresponsive to conservative and pharmacologic therapies. In a cohort of 64 patients with refractory pelvic floor dysfunction, Aboseif et al. reported that 80% experienced > 50% improvement in symptoms and quality of life after SNM [6, 59]. Anecdotally, SNM has also been associated with improvements in bowel, vaginal, neuropathic, and sexual symptoms [60].
Despite these benefits, SNM is an invasive treatment and is not FDA-approved specifically for NR-PFD. In Torosis et al., 60% of experts supported its use only in patients with coexisting urgency, frequency, or retention who have failed less invasive measures. SNM should not be used as primary therapy for isolated NR-PFD, and patients must be counseled on its off-label use and expected outcomes [42].
Integrative/Holistic Approaches: Acupuncture, At-Home Therapies, and Cognitive Behavioral Therapy
Complementary and integrative approaches may serve as valuable adjuncts, particularly in patients with persistent pelvic pain or stress-related symptom exacerbations. While data remain limited, some evidence supports the use of acupuncture in improving pain, urinary symptoms, and overall quality of life among patients with chronic pelvic floor dysfunction [61, 62].
First-line home-based therapies, including daily pelvic floor stretching, application of warm compresses, and relaxation-focused exercises such as yoga, are frequently recommended as first-line management options for patients [42]. These interventions are low-risk, accessible, and may reinforce pelvic floor relaxation and neuromuscular downregulation.
Cognitive behavioral therapy (CBT) has shown benefit in NR-PFD patients with chronic pelvic pain or psychosexual dysfunction. Its utility lies in targeting central sensitization, maladaptive coping, and psychosocial contributors [63, 64]. In Torosis et al., 80% of experts supported incorporating psychological counseling or CBT into the treatment algorithm, typically as a second-line option following PFPT [42].


Comments (0)