
Remember me
This study was conducted at the Veterans Health Service Medical Center in Seoul, Republic of Korea, between July and December 2023. Participants were recruited through convenience sampling during routine clinical visits, and eligibility was determined by trained clinicians based on predefined inclusion and exclusion criteria. Inclusion criteria were: (1) age ≥ 60 years; (2) ability to ambulate independently and communicate verbally; (3) absence of major neurological or systemic medical conditions that could influence prefrontal cortical hemodynamics, including cancer, prior cerebral infarction or hemorrhage, Parkinson’s disease, or other progressive neurodegenerative disorders; and (4) absence of physician-diagnosed depression or current use of antidepressants. Individuals with subjective concerns of cognitive decline, but without a formal diagnosis of dementia, were also eligible. Exclusion criteria included: severe mobility impairments precluding safe task performance, inability to complete the verbal fluency task, or technical issues preventing reliable acquisition of fNIRS data.
Based on these criteria, a total of 314 community-dwelling older adults provided informed consent and were enrolled. Of these, 6 participants were subsequently excluded due to incomplete or unreliable fNIRS data (e.g., sensor detachment, drowsiness during testing, or device malfunction). The final analytic sample therefore comprised 308 participants.
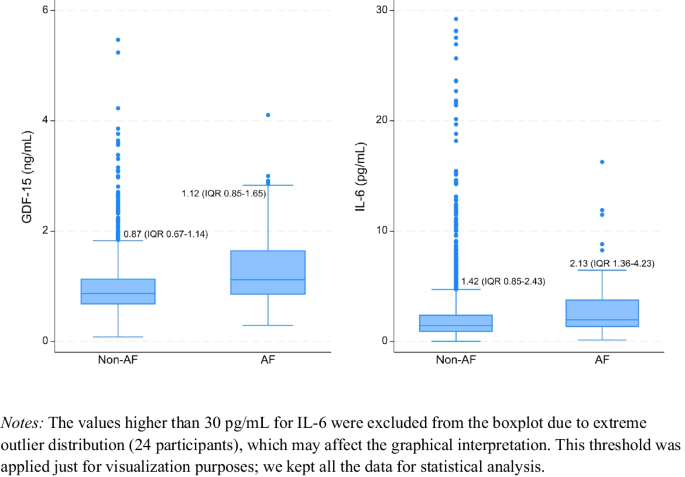
fNIRS data acquisition and preprocessingA portable continuous-wave fNIRS device (NIRSIT Lite Adult; OBELAB, Inc., Seoul, Korea) was used to measure hemodynamic responses in the PFC during the task. The system included 15 channels with a 3 cm source-detector distance and used dual wavelengths (780 and 850 nm) at a sampling rate of 8.138 Hz. It was also equipped with two short-separation channels, one in each hemisphere, with a source-detector distance of 0.8 cm. The device primarily targeted the anterior PFC (BA10), approximately covering adjacent regions including the dorsolateral and ventrolateral PFC. Figure 1 illustrates the configuration of the channels and their estimated positions on the automated anatomical labeling (AAL) atlas [20].
Fig. 1
Channel configuration of the fNIRS device. The estimated positions of sources (green dots) and detectors (blue dots) are superimposed on the AAL brain atlas. Each source-detector pair comprises fifteen regular channels (numbered magenta dots) and two short-separation channels (smaller magenta dots). The majority of measurement channels were positioned over the anterior prefrontal cortex, with some (channels 1 and 15) located over the inferior frontal gyri
During fNIRS data acquisition, participants performed a verbal fluency task using a tablet PC that presented the instructions and stimuli. The task consisted of two cycles, each comprising three sequential phases. In each cycle, participants first engaged in a 30-s resting period, during which they were instructed to fixate on a central cross displayed on the screen. This was followed by a 30-s control condition, where they repeatedly uttered vowels (“a, e, i, o, u”) aloud. Finally, in the 30-s task condition, participants were presented with an initial Korean consonant (‘Giyuk’ in the first cycle and ‘Siot’ in the second cycle) and asked to generate and verbally produce as many words as possible beginning with the presented consonant.
The preprocessing steps for the fNIRS data were as follows. First, channels with low signal quality due to saturation or severe motion artifacts were excluded from the analysis [35]. Specifically, the raw light intensity signal in each channel was examined and removed if it met any of the following criteria: (1) contained signs of saturation (more than five negative values in a row or the same consecutive value persisting for more than 5% of the entire time series); (2) showed weak net signal (median intensity lower than 30 A.U.); (3) exhibited signs of noise (a coefficient of variation greater than 7.5% in more than 10% of 5-s intervals [2]; or (4) demonstrated severe negative correlation between HbO and deoxyhemoglobin (HbR) concentrations [28]. Second, the raw signals were converted to optical density and corrected for motion artifacts using the Temporal Derivative Distribution Repair (TDDR) algorithm [8]. Third, the corrected optical density values were converted to changes in hemoglobin concentration via the modified Beer-Lambert law [6, 7]. For this conversion, the molar extinction coefficients reported by Zhao et al. [36] were applied, with no differential pathlength factor, resulting in hemoglobin concentration units of mM·mm [36]. Finally, data were bandpass filtered between 0.005 and 0.1 Hz to remove frequencies of no interest such as cardiac pulsation and slow drifts. Overall, less than 1% of the total observations were rejected during preprocessing, and these were replaced by the mean of nearby channels. All preprocessing and subsequent statistical analyses described in the next section were performed using NIRSIT Quest software (version 1.0.0; OBELAB, Inc., Seoul, Korea).
fNIRS data analysisTo quantify and summarize brain activation during the verbal fluency task, a general linear model (GLM) was applied to the hemoglobin signals. Beta coefficients were estimated using the Ordinary Least Squares (OLS) method [9]. The design matrix included main regressors modeling the task condition (verbal fluency) and the control condition (vowel utterance), along with their temporal and dispersion derivatives to account for variability in response timing. To further improve model fit and reduce confounding influences, nuisance regressors were incorporated. Any residual motion artifacts were addressed by including three head movement angle estimates (rotation in x, y, and z directions) derived from the inertial measurement unit (IMU) sensors [18]. Additionally, signals from short-separation channels were averaged and included as nuisance regressors to remove superficial physiological noise [10, 31]. The model was independently fitted to the concentration changes in.
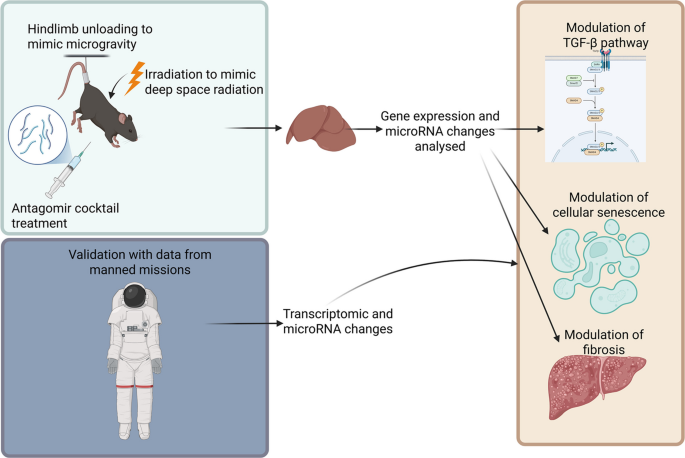
HbO and HbR. Task-related prefrontal activation for each participant was defined by combining the parameter estimates using a contrast vector of [1–1], representing Task versus Control. Channel-wise contrasted beta estimates were computed and summarized at the regional level by averaging estimates across predefined regions of interest (Fig. 2). For details regarding ROI definitions, see OBELAB Inc. ([16]) (Obelab Inc, [16]). We primarily focused on HbO results, as previous studies have demonstrated that HbO generally provides a higher contrast-to-noise ratio compared to HbR [26].
Fig. 2
Pre-defined regions of interest based on channel clustering. Activation in each channel was summarized across channel groups defined by hierarchical clustering of functional connectivity patterns derived from an independent dataset (excerpted with permission from OBELAB Inc. [16])
Assessment of FoFFear of falling was measured using the Korean version of the ABC scale, a validated instrument that assesses individuals’ confidence in performing 16 common daily activities without losing balance. These activities encompass a range of scenarios such as walking indoors and outdoors, reaching overhead, navigating stairs, and using escalators. Participants rated their confidence for each item on a scale from 0 (no confidence) to 100 (complete confidence), and the final ABC score was calculated as the average of the 16 items [19]. Higher scores indicate greater balance confidence and therefore lower levels of FoF.
The Korean version of the ABC scale has demonstrated strong psychometric properties. Its translation fidelity was confirmed via a forward–backward translation procedure, and previous studies have reported high internal consistency (Cronbach’s α = 0.96) and concurrent validity with other fall-related measures such as the Falls Efficacy Scale (Spearman’s ρ = 0.78, p < 0.01), supporting its use in Korean older adult populations [12].
Variables of interestDemographic and health-related covariates were included to contextualize the relationship between cerebral hemodynamics and balance confidence. Age was categorized into six groups (60–64, 65–69, 70–74, 75–79, 80–84, and ≥ 85 years). Other variables included sex (male or female), marital status (married, widowed, divorced, or never married), and educational attainment (less than high school vs. high school or more). Smoking status was self-reported as current, former, or never smoker. Participants also indicated whether they had ever experienced a fall (yes or no). Clinical comorbidities were identified based on self-reported physician diagnoses of hypertension, dyslipidemia, and diabetes mellitus. Additionally, the number of medications currently taken was recorded and categorized as 0, 1, or ≥ 2. Global cognitive function was evaluated using the Mini-Mental State Examination (MMSE), a widely used screening tool for cognitive impairment in older adults. The MMSE assesses orientation, attention, memory, language, and visuospatial skills, with scores ranging from 0 to 30, where higher scores reflect better cognitive performance. This measure was included as a covariate to account for potential confounding, given that cognitive status may influence both FoF and PFC activation during the verbal fluency task.
Statistical analysisWe hypothesized that prefrontal hemodynamic activity—indexed by HbO measured via fNIRS—would be positively associated with balance confidence in older adults. To test this hypothesis, we performed both unadjusted and multivariable linear regression analyses, using HbO concentrations in predefined frontal cortical regions as independent variables and ABC scores as the continuous dependent outcome. The fully adjusted model controlled for potential confounders, including age, sex, marital status, education level, smoking status, fall experience, chronic disease history (hypertension, dyslipidemia, diabetes), medication count, and cognitive function. Beta coefficients and standard errors (SE) were estimated to quantify the association between HbO levels and ABC scores.
In addition, we conducted subgroup analyses stratified by fall history, age group, sex, and educational attainment to examine whether the association between PFC activation and balance confidence varied across key sociodemographic and clinical characteristics. For each subgroup, both unadjusted and adjusted linear regression models were estimated to assess the consistency and robustness of the associations. These analyses aimed to identify potential effect modification by vulnerability factors known to influence both FoF and cortical activation patterns. To enhance visualization of cortical activation contrasts, we additionally illustrated the most extreme subgroups, defined as participants with high ABC scores (≥ 80) and those with low ABC scores (≤ 40). This stratification was applied solely for graphical presentation and was not used in the main statistical analyses.
All statistical analyses were performed using SAS version 9.2 (SAS Institute, Cary, NC, USA), and statistical significance was defined as a two-tailed p-value < 0.05.
Comments (0)