
Remember me
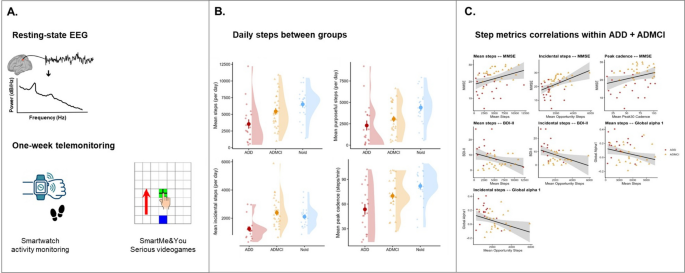
Participants included in this study were consecutively enrolled from clinical units participating in the national PREDICT-NEURODEGEN project. Initially, 89 individuals underwent the study procedures, including 25 individuals with Alzheimer’s disease dementia (ADD), 35 with mild cognitive impairment due to Alzheimer’s disease (ADMCI), and 29 cognitively unimpaired older adults (Nold). All participants underwent an intake interview. For the ADD and ADMCI groups, this was preceded by a routine neurological examination. Study procedures then included neuropsychological testing, resting-state EEG recordings, and one-week home telemonitoring using Samsung Galaxy Watch 4–6 smartwatches and the SmartMe&You-TELEMAIA application (https://smartme.cloud.garr.it/en/) installed on a commercial tablet. EEG protocols and telemonitoring procedures are detailed in the following sections.
The diagnosis of AD in participants belonging to the ADD and ADMCI groups was based on a history of gradual cognitive decline supported by established biomarkers. Specifically, AD status was assigned based on positivity (i.e., abnormal findings indicative of amyloid pathology, tau pathology, and/or AD-related neuronal injury) on one or more of the following examinations: Aβ1–42/phosphotau ratio in cerebrospinal fluid (CSF) or blood serum, ^18F-fluorodeoxyglucose positron emission tomography (FDG-PET), and structural magnetic resonance imaging (MRI) showing involvement of the hippocampal, parietal, temporal, and posterior cingulate regions [39]. Regarding cognitive status, the additional classification of dementia (ADD) or mild cognitive impairment (ADMCI) was assigned according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria [40]. ADD was defined by major cognitive decline reported by the patient or informants, or observed by clinicians, with significant impairment in at least one cognitive domain documented by neuropsychological testing and reflected by performance below normative reference values (i.e., scores falling more than 1.5 standard deviations below the mean for age- and education-matched controls, or standardized scores indicating abnormality relative to population norms), together with loss of autonomy and moderate-to-severe impairment in instrumental activities of daily living. ADMCI was defined using the same criteria, except for the preservation of functional autonomy in activities of daily living. In both groups, cognitive decline was not attributable to other medical or psychiatric conditions, and other major neurological or psychiatric diagnoses, including mixed dementing conditions, were excluded during clinical examination. In addition, at study inclusion, participants with ADD or ADMCI could not be enrolled in clinical trials involving experimental drugs, nor be receiving antidepressants with anticholinergic side effects, high doses of antipsychotics, chronic sedative/hypnotic treatment, antiparkinsonian medication, or narcotic analgesics.
Nold participants showed no evidence of cognitive impairment on neuropsychological testing, did not report any current or past major medical, neurological, or psychiatric condition, and were not taking psychotropic medications chronically at the time of the study.
Additional exclusion criteria for all groups included the presence of a severe depressive episode, defined as a score > 20 on the 30-item Geriatric Depression Scale [41] or > 28 on the Beck Depression Inventory-II [42], as well as the presence of chronic systemic illnesses such as diabetes mellitus.
Global cognitive functioning was assessed using the Mini-Mental State Examination (MMSE) [43]. A comprehensive neuropsychological assessment was then conducted using the test batteries available at each recording unit, covering the core domains of memory, attention and executive functioning, language, and visuospatial abilities. Long-term verbal memory was assessed using short story recall [44] and the Rey Auditory Verbal Learning Test [45], while long-term visuospatial memory was evaluated using delayed recall of the Rey-Osterrieth Complex Figure [46]. Attention and executive functioning were assessed with the Trail Making Test, including Parts A and B and the B-A index [47]. Visuoconstructional abilities were examined using the immediate copy of the Rey- Osterrieth Complex Figure [46] and the Clock Drawing Test [48]. Language abilities were assessed using phonemic (letters F, P, and L) and semantic (animals, fruits, and car brands) verbal fluency tasks [49].
Autonomy in daily functioning was assessed using Katz’s Index of independence in activities of daily living (ADL) [50], which evaluates independence in six basic activities (e.g., personal hygiene and dressing), with a maximum score of 6 indicating full autonomy. Instrumental functioning was assessed using Lawton’s instrumental activities of daily living (IADL) scale [51], which rates independence across eight more complex activities (e.g., meal preparation, telephone use, and financial management), with higher scores indicating greater functional autonomy. For both instruments, information was obtained either directly from the participant or from an informant/caregiver, depending on the participant’s clinical condition and degree of cognitive impairment.
Daytime sleepiness was assessed using the eight-item Epworth Sleepiness Scale (ESS) [52]. Depressive symptoms were evaluated using the 21-item Beck Depression Inventory-II (BDI-II) [42] or, in some cases, particularly among cognitively unimpaired participants, the 30-item Geriatric Depression Scale (GDS) [41], depending on the clinical protocol of the recruiting unit.
The study was approved by the local institutional ethics committees of the recruiting units. All procedures were conducted after informed consent had been obtained from each participant or caregiver, in accordance with the Declaration of Helsinki (2013 revision) and the standards established by the local institutional review boards.
SmartMe&You-TELEMAIA serious videogamesThe SmartMe&You-TELEMAIA application was designed for home-based telemonitoring of cognitive functions and includes a set of serious videogames grounded in neuropsychological models of vigilance and attention developed by researchers at Sapienza University of Rome (https://smartme.cloud.garr.it/en/). The cognitive battery comprises seven unsupervised tasks that can be administered on a commercial tablet, and a short video demonstration of the serious videogames is available online at: https://www.youtube.com/watch?v=wfBm7WxX_RY.).
All tasks are based on the same visual grid displayed on the tablet screen, consisting of 7 × 7 black squares on a white background. Across tasks, cue stimuli and green “go” stimuli are presented on the screen, and participants are required to respond by touching the go stimulus with the dominant finger, initially positioned on a starting blue square, as accurately and quickly as possible. Figure 1 illustrates the common response procedure underlying the SmartMe&You-TELEMAIA tasks and shows an example of the application interface used to provide visual instructions.
Fig. 1
Illustration of the SmartMe&You-TELEMAIA serious videogame interface and response procedure. A Schematic representation of the basic task layout used across the battery, showing the 7 × 7 visual grid, the central fixation cue, the starting blue square, and the required touch response to the green “go” stimulus followed by return to the starting position. B Example of the application interface presenting the step-by-step visual instructions for Task 1 on the tablet screen. The screenshot is shown in its original Italian-language version
The first two videogames are simple sustained visual reaction-time tasks using a central green target (“go” stimulus) presented with randomly varying inter-trial intervals, shorter in Task 1 and longer in Task 2. Both tasks assess the ability to maintain tonic vigilance across trials and to execute rapid, coordinated visuomotor responses. The third videogame presents non-spatial warning cues, consisting of brief whole-screen brightening preceding some of the go stimuli, and assesses responsivity to prompting. The next two videogames (Tasks 4 and 5) implement different variants of the standard Posner task to assess visuospatial attention. In these tasks, valid spatial cues indicate the side of the grid (left or right) on which the green go stimulus is likely to appear, with different assigned probabilities; accordingly, validly cued targets are expected to elicit faster reaction times than invalidly cued ones. Another videogame implements an inhibition-of-return condition, in which a pseudo-cue serves as a non-informative spatial cue with a random 50% probability of correctly predicting the side of appearance of the go stimulus. Under this condition, reaction times are expected to be slower for go stimuli appearing on the same side as the pseudo-cue, corresponding to the inhibited spatial area. The final videogame is a visual go/no-go task in which green go and red no-go stimuli appear centrally, testing the ability to respond selectively to go stimuli while inhibiting impulsive responses to no-go signals.
Throughout all tasks, the application records response timing (millisecond reaction times) and accuracy (percentage of correct responses), as well as whether participants maintained finger contact with the starting blue square during non-response intervals. Each task includes a specific number of trials depending on the customizable experimental configuration. Visual cues and short textual messages at the beginning and end of each task mark transitions and help participants remain engaged and informed about successful task completion. Performance data are transmitted in real time to the web-based SmartMe&You-TELEMAIA platform hosted on the GARR Consortium cloud infrastructure (https://garr.it/), where they are stored, accessed, and processed by the research team.
For the analyses performed in the present study, we extracted and processed the global SmartMe&You-TELEMAIA serious videogame accuracy and reaction-time indices, computed as the mean of valid metrics across the seven tasks. Because formal external validation of the platform is still ongoing, these indices were treated as experimental ecological markers of cognitive performance rather than as substitutes for standardized neuropsychological tests.
Smartwatch-based telemonitoring of physical activityFollowing the rsEEG session, participants received a Samsung Galaxy Watch 4–6 smartwatch and were instructed to wear it continuously for one week, charging the device around lunchtime and refraining from interacting with the application functions. Device return was scheduled approximately seven days later, depending on participants’ availability. Mean monitoring duration across participants was 7.0 ± 1.2 days. When necessary, caregivers were involved to support proper and continuous device use.
In the present study, step count data recorded at one-minute resolution by the smartwatch accelerometer and stored in the Samsung Health application were analyzed. Previous investigations have demonstrated good validity of Samsung smartwatches for estimating step counts under freeliving conditions in adult populations [53, 54].
At the end of the monitoring period, step count data were exported via the Samsung Health application and stored as raw CSV files. For each participant, four summary indices were computed and averaged across the entire monitoring period, capturing both activity volume and activity intensity in line with prior large-scale epidemiological studies [8]. Specifically, the following metrics were derived: mean daily steps over 24-h periods; mean daily purposeful steps, defined as steps accumulated at a cadence ≥ 40 steps/min; mean daily incidental steps, defined as steps accumulated at a cadence < 40 steps/min; and mean peak 30-min cadence, defined as the average steps per minute across the 30 highest-cadence minutes of each day, not necessarily consecutive.
To reduce the influence of incomplete monitoring days (e.g., device return in the morning), a datadriven quality-control procedure was applied to minimize bias due to partial wear without arbitrarily excluding valid low-activity days. Days with extremely low step counts (< 200 steps/day) were excluded. In addition, the last recorded day was removed when its total step count was lower than 35% of the median daily step count across the remaining monitoring days, provided that at least three valid days remained available for averaging. Participants with fewer than three valid monitoring days after these quality-controls were excluded from all analyses performed in this study.
Resting-state EEG acquisitionEEG recordings were conducted at each recruiting site using a standardized protocol. Participants were seated comfortably in a reclined chair in a dimly lit room, and all recording sessions were scheduled in the morning to control for homeostatic sleep pressure and minimize fatigue. To reduce acute effects on resting-state EEG activity, participants were instructed to abstain from caffeine intake on the morning of the recording and, when applicable, to delay medication intake until after the session.
Each EEG recording included at least two consecutive conditions: a resting-state eyes-closed condition lasting 3 to 5 min, depending on recording quality, and a resting-state eyes-open condition of similar duration. During both conditions, participants were instructed to remain relaxed, let their mind wander, and avoid focused mentation. Voluntary movements and speaking were discouraged. If behavioral or EEG signs of drowsiness or sleep onset emerged, such as ripples, vertex sharp waves, K-complexes, or sleep spindles, participants were gently prompted to remain awake.
Only the resting-state eyes-closed condition, reflecting quiet wakefulness, was considered for the analyses presented in this study.
At each recording unit, EEG data were acquired using local acquisition systems configured to prevent aliasing, with analog band-pass filters set between 0.01 and 100 Hz and sampling rates of 256, 512, or 1000 Hz. Monopolar montages comprising 19 or 32 electrodes based on the international 10–20 system were employed, with a frontal electrode used as ground and a cephalic reference electrode positioned according to site-specific protocols. Electrode impedances were maintained below 5 kΩ throughout the recordings.
EEG preprocessingAll EEG data were centrally analyzed by trained researchers among the study authors using procedures adopted and validated in previous EEG studies [55, 56]. The preprocessing pipeline was designed to enhance signal quality and remove physiological and non-physiological artifacts, as well as malfunctioning channels, in accordance with the guidelines for the quantitative analysis of restingstate EEG rhythms proposed by the International Federation of Clinical Neurophysiology [57].
Raw EEG data were acquired in European Data Format, reduced to a common 19-channel montage (Fp1, Fp2, F7, F3, Fz, F4, F8, T7, C3, Cz, C4, T8, P7, P3, Pz, P4, P8, O1, and O2), and processed using the EEGLAB toolbox [58] (version 2025.0.0) within the MATLAB environment (version 2024b; MathWorks, Natick, MA, USA). Preprocessing was aimed at identifying and correcting channels with persistent artifacts or excessive noise, removing contaminated signal segments across multiple electrodes, and isolating independent signal components attributable to non-neural sources.
Two researchers independently performed an initial visual inspection of each EEG trace, segmented into 2-s epochs, to identify electrodes showing continuous artifacts; a third expert was consulted in cases of disagreement. No more than three channels were removed at this stage, and missing channels were reconstructed using EEGLAB interpolation routines. Subsequently, three researchers visually reviewed the recordings to identify and reject residual segments affected by muscle activity, ocular artifacts, head movements, or other non-physiological noise. Independent component analysis was then applied to isolate residual artifactual components related to blinking, eye movements, muscle activity, and cardiac signals [59, 60]. Up to five components were removed based on consensus evaluation of their spatial topographies and spectral characteristics.
Following a final visual inspection, the cleaned EEG signals were band-pass filtered between 0.5 and 45 Hz, downsampled to 256 Hz when originally acquired at higher sampling rates, and re-referenced to the common average of all electrodes before quantitative analysis.
Spectral analysis and source estimation of resting-state EEGPower spectral density (PSD) was computed for all artifact-free eyes-closed rsEEG epochs at each scalp electrode using the Welch method with a Hanning window and no phase shift, yielding a frequency resolution of 0.5 Hz.
For each participant, two individual frequency landmarks were identified based on global and posterior average PSD profiles: the transition frequency (TF) and the individual alpha frequency (IAF) [61]. The IAF was defined as the frequency between 6 and 14 Hz at which the PSD showed the maximum alpha peak, whereas the TF was defined as the frequency between 3 and 8 Hz at which a local minimum in the PSD occurred. Based on TF and IAF, individual frequency bands were defined as follows: delta from TF—−4 Hz to TF—−2 Hz, theta from TF—−2 Hz to TF, alpha 1 from TF to the midpoint between TF and IAF, alpha 2 from that midpoint to IAF, and alpha 3 from IAF to IAF + 2 Hz.
Cortical sources of rsEEG activity were estimated using exact low-resolution brain electromagnetic tomography (eLORETA, version 2020; https://uzh.ch/keyinst/loreta.htm) [62], a distributed linear inverse solution that provides three-dimensional estimates of intracortical current density from scalprecorded EEG signals. The head model includes scalp, skull, and cortical compartments and is based on the Montreal Neurological Institute MNI152 template. Within this realistic head volume conductor model, eLORETA computes a regularized solution to the EEG inverse problem by estimating the distribution of neuronal current density at each cortical voxel.
The solution space comprised 6,239 voxels with a spatial resolution of 5 mm, restricted to cortical gray matter. Each voxel contains an equivalent current dipole representing the mean current density generated by the local population of pyramidal neurons. Talairach coordinates, lobar classification, and corresponding Brodmann areas (BAs) are provided for each voxel.
Scalp PSD values computed at the 19 electrodes were used as input to eLORETA, which returned voxel-wise current density estimates for each frequency bin between 0.5 and 45 Hz. Given the relatively low spatial resolution associated with the 19-channel montage, voxel-wise solutions were aggregated into six macro-regions of interest (ROIs): frontal (BAs 8, 9, 10, 11, 44, 45, 46, and 47), central (BAs 1, 2, 3, 4, and 6), parietal (BAs 5, 7, 30, 39, 40, and 43), occipital (BAs 17, 18, and 19), temporal (BAs 20, 21, 22, 37, 38, 41, and 42), and limbic (BAs 31, 32, 33, 34, 35, and 36).
For each individual frequency band (delta, theta, alpha 1, alpha 2, and alpha 3) and within each ROI, current density values were averaged across the frequency bins belonging to the band and log10- transformed to improve distributional properties. ROI-level values were then averaged across frontal, central, parietal, occipital, temporal, and limbic regions to obtain global indices for each band. In addition, a synthetic resting-state vigilance index was computed in line with previous suggested solutions [28, 63] as the logarithmic difference between fast- and slow-frequency activity, defined as the difference between (global alpha 2 + global alpha 3) and (global delta + global theta) current densities in log10 space.
Statistical analysisStatistical analyses were performed using jamovi (version 2.5.6) [64] and R (version 4.5.1) [65]. Continuous and ordinal variables are reported as means and standard deviations, whereas categorical variables are presented as counts and percentages. Before inferential analyses, the distributions of continuous variables were visually inspected using Q–Q plots and histograms. When substantial deviations from normality were detected, nonparametric tests were applied as appropriate. Given the moderate sample size and the relative robustness of parametric procedures to modest departures from normality, analyses were conducted under standard parametric assumptions unless clear violations were observed.
Between-group comparisons for demographic and clinical variables were performed using analysis of variance (ANOVA) or independent-samples t-tests for normally distributed variables, and Kruskal–Wallis or Mann–Whitney tests depending on the number of groups and distributional assumptions. Differences in the distribution of categorical variables were examined using chi-squared (χ2) tests.
In the main analyses, rsEEG indices, serious videogame performance measures, and smartwatchderived activity metrics were compared across groups using analysis of covariance (ANCOVA), controlling for age, sex, and education, and additionally for the number of monitoring days in the case of smartwatch-derived variables. Effect sizes were quantified using eta-squared (η2). Post hoc comparisons were corrected for multiple testing using Holm’s sequentially rejective procedure [66], and Cohen’s d was calculated as an effect size estimate for pairwise comparisons.
To examine associations among clinical, EEG, and activity variables in participants with AD, Pearson product-moment partial correlation coefficients were computed while adjusting for age, sex, and education. Given the exploratory nature of these analyses, 95% percentile bootstrap confidence intervals were estimated for each correlation coefficient using 5,000 resampling iterations with the boot R package [67] (seed = 202,603). In addition, as a sensitivity analysis, partial correlations were also computed in the full sample, including Nold participants, to evaluate whether associations observed within the AD clinical sample were sensitive to sample restriction and to describe their behavior across a broader range of variability.
To quantify the informativeness of the available sample for the exploratory partial correlation analyses involving the clinical sample, a sensitivity power analysis was conducted using G*Power (version 3.1.9.7) [68]. In line with current recommendations for sample-size justification in studies with already determined or resource-constrained samples [69], this analysis estimated the minimum effect size detectable with 80% power, using α = 0.05 and three covariates (age, sex, and education). For the full AD clinical sample (ADD + ADMCI; N = 47), the minimum detectable effect size was Cohen’s f2 = 0.175, corresponding to a partial correlation of approximately |r|≥ 0.39. For analyses involving rsEEG markers, where EEG data were available for 41 AD participants, the minimum detectable effect size was Cohen’s f2 = 0.202, corresponding to a partial correlation of approximately|r|≥ 0.41.
Moreover, in order to evaluate whether the rsEEG findings depended on the use of individually defined frequency bands, supplementary sensitivity analyses repeated the EEG group comparisons and AD clinical sample partial correlations using fixed-frequency global eLORETA bands: delta (2–4 Hz), theta (4–6 Hz), and alpha (8–12 Hz).
Finally, in dedicated supplementary analyses, neuropsychological test scores were examined across groups and in relation to activity metrics within the AD clinical sample (ADD + ADMCI) using the same procedures described above. Given the heterogeneity of neuropsychological batteries across recruiting sites, and the resulting variable-specific sample sizes, these analyses were restricted to measures administered consistently across sites. To provide preliminary evidence of convergent validity for the SmartMe&You-TELEMAIA battery, partial correlations were also computed between global serious videogame accuracy and reaction time, MMSE, and neuropsychological test scores.
For all analyses, corrected or uncorrected p values below 0.05 were considered statistically significant.
Comments (0)