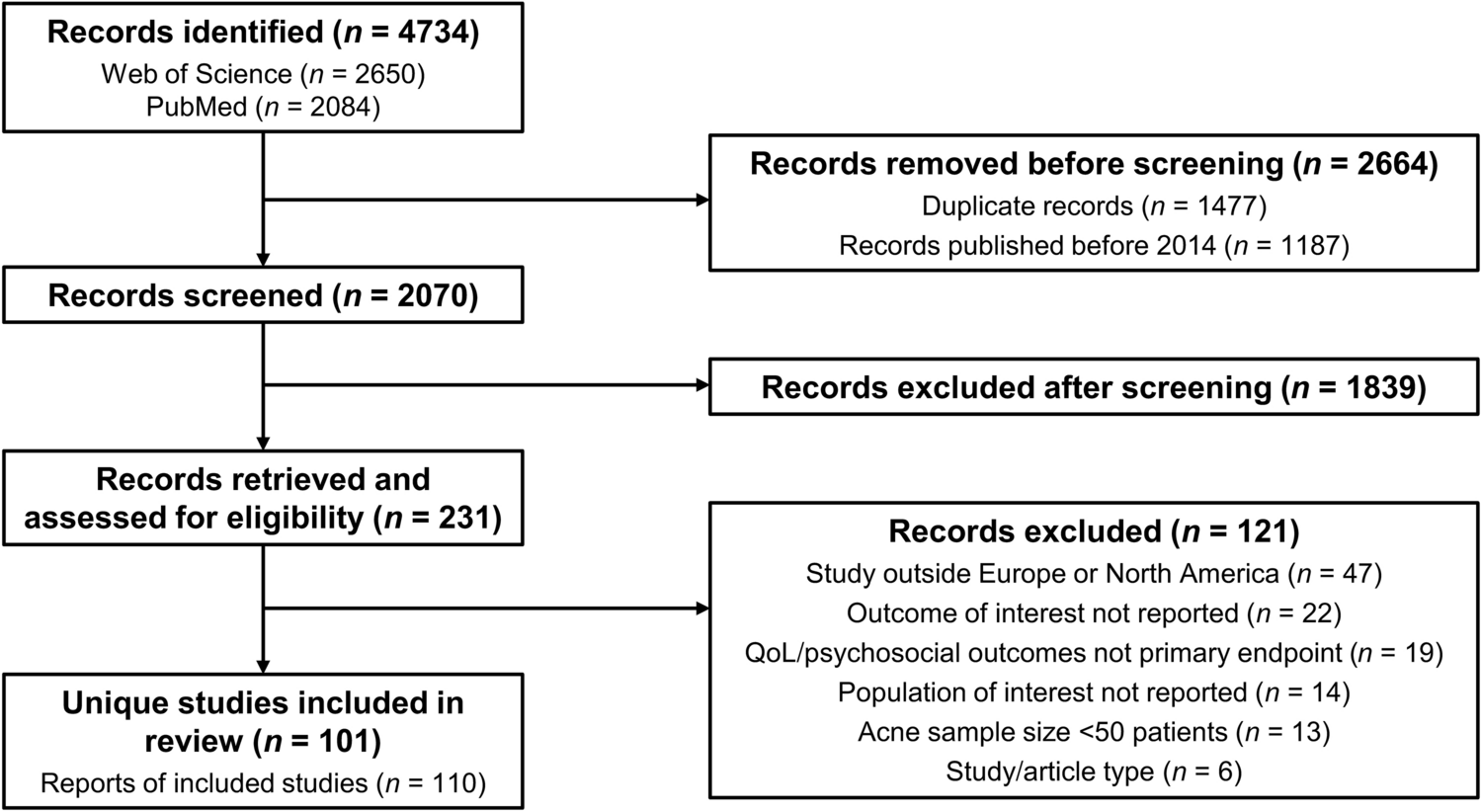
A total of 1137 articles were identified, of which 50 were selected for inclusion. Of these studies, 14 randomized controlled trials (RCTs; Table 1), 17 real-world interventional or noninterventional studies (Tables 2, 3, respectively), 11 sets of international clinical guidelines, five systematic literature reviews (SLRs), one definition validation study, and two eDelphi studies were included.
3.1 Definitions of AD Flares from SLRs of Prospective, Interventional Clinical Trials
Four SLRs were identified that examined approaches to defining flare in AD; some data used to draw conclusions across these studies were the same [15, 17,18,19]. In addition to the studies published during the search period, the foundational work published in 2006 by Langan et al., which investigated the definitions of flare used in AD clinical trials and other chronic intermittent diseases, has been included in this analysis owing to relevance to the research questions [3]. Langan et al. found 15 studies that measured and defined disease exacerbation or flare in AD. From this, the authors identified three broad themes of definition:
1.
Composite definitions comprising multiple factors, such as severity, symptoms, and treatment: for example, an Investigator’s Global Assessment (IGA) score of ≥ 4 requiring topical corticosteroids within 3 days, followed by 7 days without such therapy [20,21,22]
2.
Arbitrary thresholds or changes in severity scores: for example, a substantial worsening in SCORing AD (SCORAD; > 15-point SCORAD increase from baseline, > 50% SCORAD from baseline, among others), or IGA ≥ 3, or a Three-Item Severity score of ≥ 4 [3, 23,24,25]. In these studies identified by Langan et al., where it is defined, “baseline” referred to the start of the study period [3]
3.
Behavioral definitions (i.e., definitions based on an action): for example, a disease state requiring systemic corticosteroid use for 3 days or more, potent topical corticosteroids (TCSs), or flare-specific systemic treatment [3]
Although the studies found by Langan et al. [3] allowed identification of broad themes, the ongoing challenge of defining flare was emphasized. Composite definitions can allow for a multidimensional patient assessment by incorporating multiple factors, but they can lead to difficulties in collecting, classifying, and interpreting data. Furthermore, while definitions based on changes in score from a baseline (e.g., SCORAD and other investigator-based assessments) provide a clear measure of flare, they may not consider or reflect the realities of a patient’s experience and rely entirely upon clinical signs as per investigator’s assessment. Langan et al. acknowledge that assuming baseline represents “normal” or “stable” disease limits the conclusions that can be drawn and excludes the patient perspective [3]. In clinical trials, treatment washout periods, inclusion criteria, and the choice of study population will all affect baseline scores and may not be representative of a patient’s actual reference disease state. Finally, although behavioral definitions may integrate some elements of patient reactions, they can lack consistency owing to the variability in individual responses, subjective symptom reporting, and treatment preferences [3].
A consistent theme among the definitions reported by Langan et al. [3] is the lack of consideration for patient-reported outcome measures (PROMs) beyond those captured within the SCORAD instrument (itch and sleep loss). Indeed, the authors acknowledged that the patient “may be in the best place to judge whether their disease is well controlled for them” and, hence, highlighted the need for a balance between meaningful definitions that are understood by both the patient and the HCPs [3].While the authors proposed a definition of flare in AD as “an episode resulting in behavior such as requiring an escalation of treatment or seeking additional medical advice,” they did not mandate a specific measure for flare, instead advocating for a definition tailored to the specific objectives of each study. The authors stressed the importance of striking a balance between capturing meaningful, patient relevant-outcomes and being sufficiently sensitive to capture differences in treatment response [3].
A follow-up SLR by Langan et al. in 2014 evaluated the definitions of flare being used in prospective intervention studies of AD published from January 1993 to February 2013 [15]. The authors assessed the level at which each identified definition met prespecified criteria for a useful definition of flare. The criteria were developed upon previous HOME initiative discussions and included the feasibility to measure flare based on definition (e.g., application to various study designs and minimally resource intensive) and to record the time flare-related symptoms occur [15]. The authors identified 26 studies that provided a flare definition. Eleven definitions were based on arbitrary cutoffs for existing severity scales (e.g., SCORAD or EASI); eight used a composite definition based on an investigator’s assessment and the perceived need for treatment escalation; six used behavioral definitions based on the need for treatment modification (from the patient or physician perspective); and one considered symptoms alone, defined as unacceptable severity of itching/scratching or the onset of oozing. Only four of these 26 definitions included PROMs (limited use of daily patient diaries and patient-reported need to increase treatment) [15]. None of the definitions reported in these studies met the prespecified criteria for a useful definition of flare; importantly, no validation studies were conducted for any of the measures assessed. Despite the minor evolution in the use of PROMs to better capture patient perspective between 2006 and 2014, the integration of patient perspective into flare definitions remained limited. Therefore, the definitions identified here could not be deemed fit for purpose to capture a flare from both a patient and HCP perspective, and further research is needed [15].
Barbarot et al. [17] published findings from an SLR that investigated methods for assessing long-term disease control in RCTs published between 2000 and 2013. Their findings revealed a similar variability in approach to defining and assessing flares as seen by Langan et al. [15]. Barbarot et al. also noted the substantial lack of patient perspective [17]. Of the 101 identified trials, 26 captured data on flare. Of these, 15 studies assessed flare as the primary outcome. Arbitrary cutoffs on existing severity scales (n = 9/26) and behavioral measures (n = 6/26; typically based on the need to escalate TCS treatment according to the patient’s or physician’s perspective) were the most frequently used definitions of flare, with time to first flare and number of flares being the most frequent outcomes assessed [17]. Employing validated severity scales may miss fundamental aspects of disease control that are important to patients and fail to distinguish between flare and gradual disease worsening, highlighting the importance of making methods relevant and applicable across all levels of disease severity and healthcare settings [17].
As part of the 2023 American Academy of Allergy, Asthma, and Immunology (AAAAI) and American College of Allergy, Asthma, and Immunology (ACAAI) Joint Task Force on Practice Parameters for AD guidelines, two SLRs and two network meta-analyses of RCTs were conducted to investigate the benefits and harms of AD-related treatments [18, 19]. A total of 104 RCTs investigating the effect of systemic treatment (60 studies) and topical treatment (44 studies) on reducing flare were identified [18, 19]. A clear definition of flare/exacerbation was consistently lacking among these trials, with some trials reporting flares as an adverse safety event, rather than as an outcome of treatment efficacy and, hence, long-term disease control. The need to separate reporting of flares from treatment-related adverse events was highlighted [18, 19]. Once again, the absence of PROMs was a consistent and common theme among the trials. The authors highlight the need to ultimately strike a balance between clinician and patient perspectives to provide a holistic, multidimensional disease assessment [19].
These previously published SLRs of flare in AD highlight the wide range of definitions used in clinical trials and other prospective settings, with many demonstrating limitations. There is need for a concerted effort among relevant stakeholders to establish a standardized framework for a definition of flare that can incorporate the patient perspective and is relevant across different healthcare settings.
3.2 Definitions of Flare in AD Clinical Guidelines
Eleven past and current clinical guidelines on the management of AD across the USA, Europe, and Asia—including guidance on flares—were identified. The American Academy of Dermatology (AAD) 2014 guidelines on the prevention of AD flares described such disease episodes as “periods of acute worsening” but stopped short of providing a precise definition. Instead, it was noted that definitions vary across studies and that this is an ongoing area of research [26]. However, a specific definition is absent from the 2023 edition on AD management with topical therapy, despite recommending flare prevention as a critical primary efficacy outcome [7, 26,27,28].
The AAAAI and ACAAI Joint Task Force published evidence-based guidelines for AD treatment in 2024; these refer to flare in AD as “active disease” and “uncontrolled disease,” which requires treatment to induce remission [29]. These definitions are vague and inappropriate, in that flares typically occur during the management of active disease, with any flares occurring during inactive disease referred to as “relapses.” However, the guideline recommendations for future research suggest to increase the emphasis on PROMs, such as RECAP [29], which is a seven-item questionnaire designed to capture the experience of disease control [30].
A position paper on the management of AD by the 2020 European Academy of Dermatology and Venereology (EADV) task force and the European Task Force on Atopic Dermatitis (ETFAD) recognized flare as a clinically meaningful term. However, the authors acknowledged the term is “difficult to delineate,” suggesting the definition of “acute, clinically significant worsening of signs and symptoms of AD requiring therapeutic intervention” [31]. This definition was mirrored in the 2022 European Guidelines on AD (EuroGuiDerm), which differed to the ETFAD definition only by the absence of “acute” [6]. Despite defining flare, the authors of both guidelines did not provide guidance on the signs and symptoms which constitute flare, nor did they define “clinically meaningful,” falling short of providing a clear measurable definition of flare for use in clinical trials.
While the 2022 EuroGuiDerm recognize the importance of the patient perspective and recommended considering it in the management of disease, they did not explicitly include a mention of patient perspective within their definition of flare [32].
The 2024 German S3 guidelines for the diagnosis and management of AD, the 2019 Middle Eastern guidelines on managing AD, and the 2021 Thai guidelines on caring for patients with AD refer to “flare” and “acute flare,” but these terms are not defined [33,34,35].
Taken together, current guidelines on the diagnosis and management of AD lack a quantifiable, patient-oriented definition of flare, in some cases avoiding a clear definition altogether or in others defining it broadly enough to allow trial designers to select appropriate measures based on individual endpoints. Guidelines also lack the patient-centricity recommended by Langan et al. (2006 and 2014), Silverberg et al. (2022), and Chu et al. (2024), suggesting that an unmet need remains for a measurable, patient-oriented definition of flare [3, 15, 29, 36].
3.3 Validating Definitions of Flare
Despite the importance of validating definitions of flare for use in clinical trials, only one such study was identified by this review. Thomas et al. [37] investigated the validity of “escalation of treatment” and “days of topical anti-inflammatory medication use” as measures of flare [37], using data from two UK-based observational studies [15, 38]. The authors found that the need to escalate treatment was intuitively understood by participants and investigators in both studies, and the proportion of days in flare correlated well with changes in other validated severity scales [38, 39]. Thomas et al. acknowledged that their study had limitations with reliability and repeatability of “self-reported escalation of treatment” as a definition of flare [37]. Regarding reliability, the authors were unable to establish whether patients interpreted the need to escalate treatment consistently within the two studies evaluated. Concerning repeatability, individualizing the approach to flare for each patient could make future comparisons and meta-analysis difficult. Moreover, the authors highlighted that the “days of topical anti-inflammatory medication use” might be influenced by the potency of topical medication used, making interpretation of results difficult [37].
Although this study validated a flare definition that was understood by patients and investigators, the definitions examined did not incorporate patient-reported outcomes and lacked the specificity and quantifiability that is required for use in RCTs. In addition, defining flare by use of topical anti-inflammatory medication is potentially flawed since the proactive, long-term, minimal-dose, intermittent application of anti-inflammatory topical agents is an established therapy for maintaining remission and decreasing risk of exacerbation in AD [27].
3.4 Patient Perspectives of Disease Flare in AD
Langan et al. [15] and Barbarot et al. [17] highlighted the importance of including the patient perspective when defining flare, rather than just relying on clinician-reported outcomes (ClinROs). Our review identified three publications (one SLR and two eDelphi studies) evaluating the elements of flare most important to patients with AD [36, 40, 41]. Silverberg et al. conducted an SLR and social media listening analysis to identify similarities and differences between patient and physician interpretation of AD burden [36]. The authors identified 1519 publications (between 2000 and 2022) and more than 3,000,000 patient/carer social media mentions (between 2018 and 2020) related to topics and terms associated with quality of life (QoL) in patients. The social listening analysis found “flare” to be the most prevalent topic with 31,180 mentions. Flare was frequently associated with negative sentiment, which was often driven by patient concern regarding pain (17,167 mentions), dry skin (13,903), itch (6061), and excoriation (4422). Conversely, out of the 1519 publications identified, fewer than 50 mentioned flare-related terms. The authors concluded that, while flare and pain are common terms used by patients with AD, there is discordance between patient sentiment and the scientific literature, highlighting the importance of considering the patient perspective [36].
The National Eczema Association (NEA) ran focus groups with a total of 29 US adults with AD (who had at least one self-reported flare in the past year) as part of an eDelphi study to define flare in AD from the patient perspective [40]. Findings revealed that patients did not relate to existing published definitions of flare and stated that quantitative measures of skin symptoms and clinical terminology did not resonate with their lived experiences of flares. Instead, six concepts important to a patient-centric definition of flare were identified: changes from patient’s baseline/normal; mental/emotional and social consequences; physical changes in skin; an all-consuming focus on the disease; the itch–scratch–burn cycle; and control/loss of control of QoL. Some of these concepts are reflected in the RECAP tool, which relates to overall long-term disease control rather than flare specifically. The authors concluded that a definition of flare in AD informed by the patient perspective could have benefits not only in clinical trials, but also in everyday clinical practice, through improving patient–provider relationships and supporting shared decision-making [40].
More recently, the same group conducted interviews and a modified eDelphi consensus process with 657 US adults with AD, to identify the components essential to a patient-centered definition of an AD flare [41]. Statements that reached the highest level of consensus were: [Flare is] “when my symptoms take significantly more of my attention than normal”; “a worsening of physical symptoms associated with AD”; and “a worsening of itching associated with AD.” While the large majority (79.7%) of participants indicated that at least one of the previously published definitions of AD flare did not resonate with them, 52.9% agreed with their HCP on how they defined flare (details on how the HCP defined flare not reported) and also reported that their definition did not change [41]. Almost all (95.1%) of the participants reported that a patient-centered definition of AD flare would be useful to them when communicating with their HCP (77.6%), managing their symptoms (67.5%), and explaining their condition to their family (49.2%) [41].
Taken together, these findings suggest that patients would support and value a definition of flare that includes their perspective.
3.5 Defining Flare in RCTs and Real-World Studies
Thirty-one studies, including 14 RCTs, six real-world interventional studies (RWISs), and 11 real-world noninterventional studies (RWNISs), published between 2014 and 2024 referencing flare in AD were identified for this SLR (Tables 1, 2, 3). Elements that formed part of the definition of flare, such as clinician-reported outcomes, patient QoL impact, itch, and a component of time, were analyzed.
3.5.1 Clinician-Reported Outcomes
Of the studies that defined flare, most used an objective ClinRO to measure flare (Tables 1, 2, 3). Clinician-determined worsening of disease that required escalation or intensification of treatment was the most used measure of flare across all three trial types (RCT, RWIS, and RWNIS) [42,43,44,45,46,47,48,49,50,51]; however, the degree of worsening was not always defined. A Physician Static Global Assessment or IGA ≥ 2 (described as “slight but definite erythema [pink], slight but definite induration/papulation, and/or slight but definite lichenification, no oozing or crusting” [52]) was used as the measure of flare in 4/31 studies (two RCTs and two RWNIs) [53,54,55]. In two RCTs, IGA was used in combination with a loss of response to treatment (defined as ≥ 50% loss of initial EASI response) to define flare [42, 56]. EASI on its own was used in two studies, defining flare as an “increase of EASI by 6–7 points” or as a “worsening of EASI by 25% from baseline” [57, 58]. A change in the SCORAD index from baseline was used as a measure of flare in four RCTs and one RWI [


Comments (0)