
Remember me
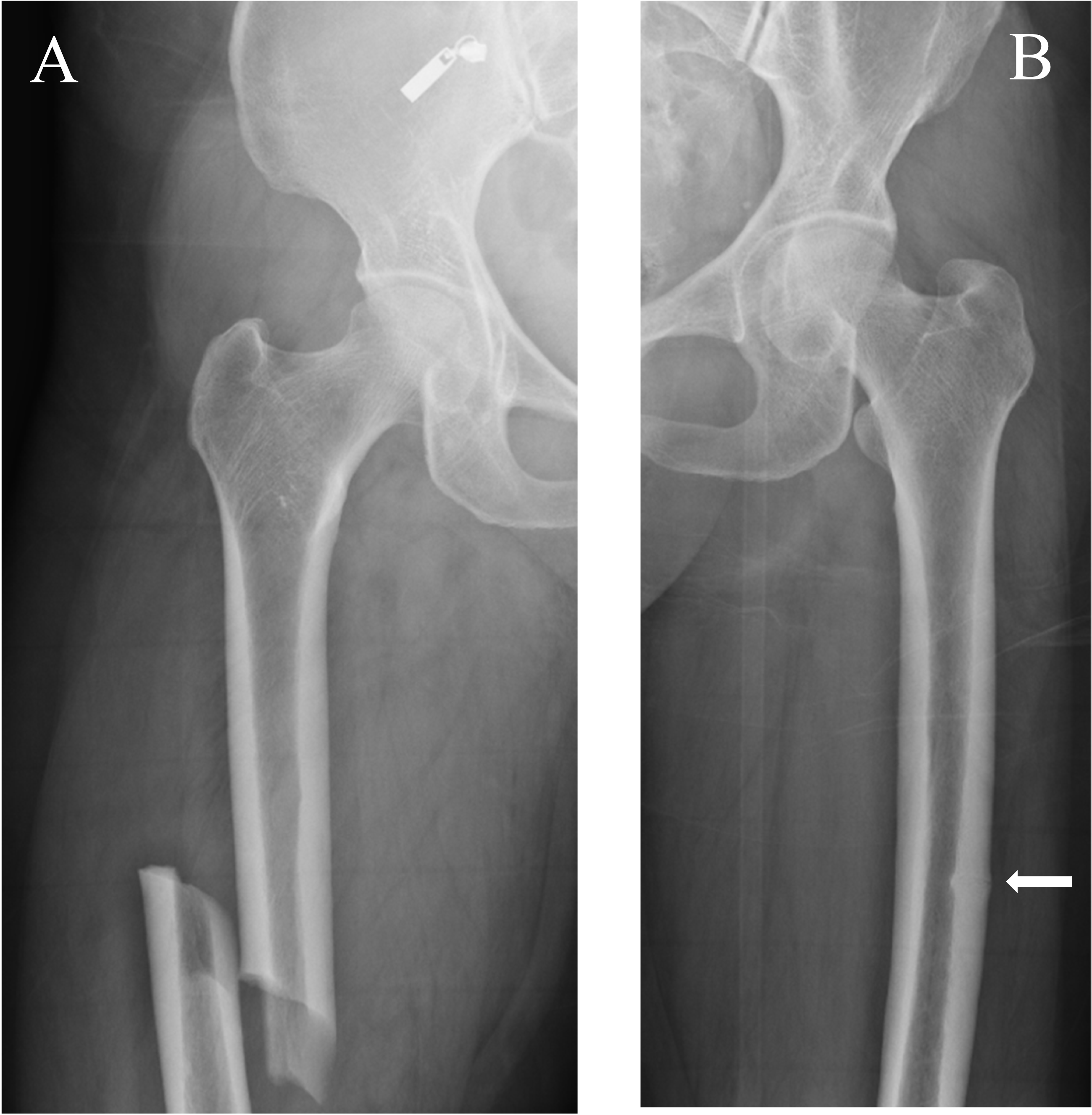

Atypical femur fractures (AFFs) were initially described in a pivotal case series of insufficiency fractures in 2005 [1]. Nine patients, receiving long-term alendronate treatment (3–8 years), sustained a variety of atraumatic fractures, including femoral shaft fractures. The American Society for Bone and Mineral Research (ASBMR) Task Force proposed a case definition for these atypical fractures affecting the femoral diaphysis in 2010 [2]. The definition was revised in 2013 (Table 1) [3]. An updated ASBMR Task Force AFF case definition is currently in development, with publication anticipated in 2026. AFFs are classically transverse in orientation, minimally comminuted and characterized by localized thickening of the lateral cortex at the fracture site, which represents their origin as a stress fracture. These radiographic features distinguish them from typical osteoporotic femoral fractures, and they may be complete or incomplete (Fig. 1).
Table 1 ASBMR task force revised case definition of AFFs [3] To satisfy the case definition of AFF, the fracture must be located along the femoral diaphysis from just distal to the lesser trochanter to just proximal to the supracondylar flare. In addition, at least four of five Major Features must be present. None of the Minor Features is required but have sometimes been associated with these fracturesFig. 1
A 58-year-old woman with osteoporosis who presented with bilateral AFFs. (A) Anteroposterior radiograph of the right femur shows a complete AFF. (B) Anteroposterior radiograph of the left femur shows an incomplete AFF (white arrow)
AFFs have been reported in anti-resorptive treated individuals, families, bisphosphonate-naïve individuals and individuals with monogenic bone diseases. Whilst anti-resorptive medications, bisphosphonates and denosumab, are effective in the management of osteoporosis, evidence has demonstrated that the risk of sustaining an AFF increases with longer duration of treatment [4, 5]. Despite this, the overall incidence of AFF is low [5]. Furthermore, the occurrence of AFFs in families, untreated individuals and those with an underlying monogenic bone disease has sparked speculation about a genetic contribution to AFF susceptibility [6, 7]. Additional postulated risk factors include younger age, Asian ethnicity, higher body-mass index (BMI), rheumatoid arthritis, varus proximal femoral geometry, lateral femoral bowing and the use of systemic glucocorticoids [3, 8, 9].
This review focuses on recent publications addressing the epidemiology, pathogenesis and management of AFFs. Emerging areas of interest, including genetic and ethnic risk factors and advancements in diagnostic technologies for AFFs, are explored.
Update on EpidemiologyIn order to ascertain an accurate estimation of AFF incidence and the increase in risk attributable to bisphosphonate therapy, longitudinal cohort studies adjudicating AFFs based on the ASBMR AFF case definition are critical [3, 5, 10]. Numerous previous studies have used International Classification of Disease (ICD) codes to diagnose subtrochanteric and femoral shaft (ST/FS) femoral fractures. However, only a small proportion of ST/FS are AFFs [5]. In recent years, key limitations have been addressed through the publication of several large longitudinal cohort studies that use ASBMR-adjudicated definitions of AFF. These studies offer substantial improvement to our understanding of the relationship between bisphosphonate exposure and AFF risk, the impact of drug holidays on AFF risk and the relationship of numerous clinical factors to AFF development [4, 11].
Duration of Bisphosphonate Use and AFF RiskThe likelihood of developing an AFF increases with prolonged exposure to bisphosphonate therapy [4, 11]. In a Southern Californian cohort (n = 196,129) of women 50 years of age or older receiving bisphosphonate therapy, 277 AFFs were detected following radiographical adjudication using the 2014 ASBMR case definition of AFFs (1.74 fractures per 10,000 patient-years) [11]. Following multivariable adjustment, compared with < 3 months of use, 3–5 years of bisphosphonate exposure was associated with an 8-fold increased risk of AFF (HR 8.86, 95% CI: 2.79, 28.20). The hazard ratio for 8 years or more of bisphosphonate use was 43.51 (95% CI: 13.70, 138.15). A recent Danish case cohort study utilising Danish National Healthcare records and blinded radiology review, found that compared with < 1 year of use, >3 to 5 years of bisphosphonate use was associated with an almost 4-fold increased risk of AFF (HR 3.94, 95% CI: 1.60, 9.65) and 5 to 7 years of bisphosphonate use was associated with a 7-fold increase in AFF risk (HR 7.29, 95% CI: 3.07, 17.30) [4]. The hazard ratio for 7 years or more of bisphosphonate use was 8.94 (95% CI: 3.92, 20.50). Interestingly, in this study “ever-use of bisphosphonate therapy” was added as a covariate to the multivariate models. Analyses performed without adjustment for any prior bisphosphonate use yielded hazard ratios more consistent with those reported by Black et al. (19.3 for 3–5 years of bisphosphonate use and 43.9 for > 7 years of use) [11]. Number needed to harm (NNH), and number needed to treat (NNT) were also evaluated. After > 5 years of anti-resorptive exposure, the NNH (for AFF development) was 1,424, whereas the NNT (for hip fracture prevention) was 56 in this Caucasian population. Extrapolated data over 10 years of anti-resorptive therapy suggested that the AFF NNH and the NNT for hip fractures began to align after a decade of use.
Drug Holidays and AFF RiskAFF risk declines rapidly following anti-resorptive discontinuation [4, 11, 12]. Black and colleagues found that rates of AFFs declined following bisphosphonate cessation: 4.50 per 10,000 person-years among current users (including ≤ 3 months since discontinuation), 1.81 per 10,000 person-years at > 3 months to 15 months since discontinuation, and approximately 0.50 per 10,000 person-years at > 15 months after discontinuation [11]. Time since bisphosphonate discontinuation was associated with a 48% reduction in the risk of AFF at > 3 months to 15 months (HR vs. ≤ 3 months 0.52, 95% CI: 0.37, 0.72) and > 74% risk reduction in subsequent years. Bauer et al. also demonstrated a reduction in AFF risk following bisphosphonate discontinuation [4]. Compared to current use, time since bisphosphonate discontinuation saw a 47% reduction in the risk AFF at > 1 to 3 years (HR 0.53, 95% CI: 0.22, 1.28) and a 77% risk reduction after > 3 years (HR 0.23, 95% CI 0.05, 1.01). These findings accord with the previous reports of Schilcher and colleagues, where a 60–70% risk reduction in AFF occurred with every year passed since bisphosphonate discontinuation (multivariable-adjusted OR 0.29, 95% CI 0.26, 0.32 in female AFF cases and 0.37, 95% CI 0.30, 0.47 in male AFF cases) [12].
Ethnicity and AFF RiskAsian ethnicity has emerged as an important risk factor for AFF [8, 9, 11, 13,14,15]. In a large population of Northern Californian women (n = 48,390), Asian women had an age-adjusted relative hazard ratio for AFF development of 8.5 compared with White women [9]. In another cohort of female bisphosphonate-users in Northern California, a large proportion (62.8%) of those who sustained an AFF were of Asian ethnicity [13]. Dhanekula et al. reported a four-fold higher proportion of Asian individuals sustained AFFs compared with typical femoral fractures (TFF) [16]. Black et al. reported an adjusted hazard ratio for AFF of 4.84 for Asian women compared with White women [11]. Similarly, we identified that Asians were 3.4 times more likely to sustain an AFF, with the highest risk seen in those of Southeast Asian ethnicity [8]. Our group also found that Asians, in particular those of Southeast Asian ethnicity, were 2- to- 3-times more likely to sustain an “earlier onset AFF” (an AFF sustained following ≤5 years of anti-resorptive use) compared with non-Asians [15]. These findings accord with a systematic review published in 2010 of 39 AFF case reports and case series, where individuals treated for ≤5 years were more likely to be of Asian origin [14].
Causes underlying the association between Asian ethnicity and AFF development remain an ongoing area of investigation. Favourable femoral geometry (smaller size, lateral bowing and smaller neck shaft angle) for AFF development in Asian individuals have been postulated to contribute. However, Dhanekula and colleagues recently found that, although Asian subjects had smaller femurs compared with non-Asians, femur neck shaft angle was similar in the Asian and non-Asian groups [16]. They purported that Asian AFF risk is independent of any ethnic specific differences in femoral geometry. Anti-resorptive drug metabolism, compliance, activity levels and genetic differences have also been thought to contribute.
Finally, the accuracy of osteoporosis diagnoses based on DXA-derived bone density T-scores, fracture risk assessment and the optimal duration of anti-resorptive treatment in Asian individuals is an evolving and controversial area. Despite the International Society for Clinical Densitometry (ISCD) recommending the use of Caucasian (non-race adjusted) normative database for all ethnic groups for T-scores, studies have demonstrated that a significant proportion of Asian women are reclassified from osteoporosis to osteopenia when using an ethnic appropriate T-score [17, 18]. In addition, recent publications by working groups representing ASBMR and the International Osteoporosis Foundation demonstrate the vast spectrum of opinions as to whether race and ethnicity should be used in fracture risk assessment [19, 20]. Lastly, it is imperative to ground these considerations in the literature, consistently demonstrating that whilst Asian individuals appear more predisposed to AFFs, they exhibit a lower likelihood of sustaining osteoporotic fractures [11, 19, 21]. Black and colleagues demonstrated that among Whites, 3 years of bisphosphonate treatment prevented 149 hip fractures and 541 clinical fractures whilst only 2 AFFs were sustained [11] (Fig. 2). Whereas for Asians, after 3 years of treatment, 8 AFFs were reported whilst only 91 hip fractures and 330 clinical fractures were prevented. Importantly, distinct to Whites, after 10 years of treatment among Asians, the number of AFFs was only slightly less than the number of hip fractures prevented. The risk-benefit profile for anti-resorptive treatment therefore appears less favourable for Asian individuals than other ethnic groups.
Fig. 2
Number of hip and clinical fractures prevented compared to AFFs associated as a function of years of bisphosphonate treatment, by race (Asian (panel A), Caucasian (panel B) and Hispanic (panel C)).
(Courtesy of New Engl J Med).
Other Osteoporosis Treatments and AFF RiskData on AFF risk associated with other osteoporosis treatments is comparatively limited relative to bisphosphonate use. A recent review identified 31 AFFs in 22 patients treated with denosumab [22]. Of these, 11 patients (15 AFF) received denosumab 60 mg 6-monthly for osteoporosis, while 11 (16 AFF) received the higher dose of 120 mg monthly for metastatic Bone disease. Notably, 8 patients sustained AFFs without prior bisphosphonate use. AFFs have also been reported following raloxifene (n = 8), although treatment sequences were often unclear [22]. Four AFFs have occurred in patients treated with romosozumab, although two of these occurred during alendronate treatment following 12 months of romosozumab treatment [22,23,24,25]. Finally, a small number of AFFs have been associated with odanacatib, a cathepsin K inhibitor that decreases bone resorption with minimal suppression of bone formation [26]. Ten patients sustained 12 AFFs (adjudicated according to the ASBMR AFF case definition) among 8,043 treated with odanacatib, while no AFFs occurred in 8,028 placebo-treated participants. This suggests mechanisms other than suppressed bone turnover may contribute to AFF pathogenesis. Overall, the current evidence is insufficient to draw definitive conclusions about AFF risk associated with non-bisphosphonate treatments. While AFFs can occur with agents such as denosumab, raloxifene, romosozumab and odanacatib, the majority of data remains centred around bisphosphonate, predominantly alendronate, therapy.
Additional Clinical Risk Factors for AFFAdditional risk factors for AFF development include glucocorticoid use, proton-pump inhibitor (PPI) use, younger age, and increasing weight. Black and colleagues reported a greater than 2-fold increased risk of AFF in those having used glucocorticoids for ≥ 1 year compared to no use (HR 2.28, 95% CI: 1.52, 3.43) [11]. Bauer et al. found that AFF risk increased 7%, 22% and 40% after 1, 3 and 5 years of glucocorticoid treatment respectively [4]. Additional AFF risk factors reported by Black et al. include decreasing height (adjusted HR per 5-cm decrement 1.28, 95% CI: 1.15, 1.43), increasing weight (adjusted HR per 5-kg increment 1.15, 95% CI: 1.11, 1.19) and younger age (adjusted HR for 65 to 74 years vs. >85 years 2.76, 95% CI: 1.62, 4.72) [11]. A modest increased risk associated with PPI use was reported (HR 1.05 per year of use, 95% CI: 1.01, 1.08) by Bauer and colleagues [4].
Anti-resorptive TreatmentWhile AFFs have been reported with denosumab use [27,28,29], the majority of cases occur in the context of bisphosphonate therapy, particularly with oral bisphosphonates, and most notably with alendronate [2,3,4, 30]. This likely reflects, at least in part, global prescribing trends: alendronate is one of the most widely prescribed anti-resorptive therapies for osteoporosis worldwide [31, 32]. Assessing AFF risk associated with other treatment options (such as zoledronate, denosumab etc.), is complicated by two main limitations. Firstly, their use is less common, limiting the absolute event numbers to study. Secondly, patients may transition to these treatments following alendronate therapy, thereby making it difficult to determine whether AFF risk should be attributed to the current treatment or the preceding bisphosphonate exposure. Additional, variations in bisphosphonate pharmacology may influence AFF risk. Differences in hydroxyapatite binding and inhibitory potency for farnesyl diphosphate synthase (FPPS) can affect the potency and duration of action of bisphosphonates [33]. Capacity for binding to hydroxyapatite appears to lie in the following order: alendronate > etidronate > ibandronate > zoledronate > risedronate. Alendronate demonstrates strong hydroxyapatite binding and moderate inhibition of FPPS, with its higher bone uptake potentially explaining its greater and longer lasting suppression of bone turnover compared with lower-affinity analogues like risedronate. The extent to which these pharmacological effects influence variations in AFF risk among anti-resorptive treatments has yet to be elucidated.
Periprosthetic FracturesThe ASBMR Task Force 2010 and 2013 AFF case definitions specifically excluded periprosthetic atypical femoral fractures (PAFF) [2, 3]. However, a growing body of evidence suggests that certain periprosthetic femoral fractures (PFF) may exhibit atypical features, particularly in patients receiving long-term bisphosphonates [34, 35] A recent systematic review evaluated 17 patients from 12 studies who sustained PAFFs following hip arthroplasty [36]. All patients were female, and all were taking bisphosphonates at the time of atypical fracture, most frequently alendronate. Like AFFs, the majority (90%) of patients reported prodromal symptoms prior to fracture. All complete PAFFs radiographically demonstrated at least four ASBMR Task Force criteria for AFF (location, transverse fracture line, non-comminuted and medial spike) [3]. Makkar et al. reported a 1.3% prevalence of PAFFs amongst ICD-coded periprosthetic hip fractures in a cohort of American Veterans aged 50 years or older who had at least one filled anti-resorptive prescription (90% male cohort, mean age at fracture 76 ± 9.5 years) [37], whilst Leclerc et al. reported a frequency of PAFFs of 8.3% amongst PFFs (> 70% occurred in women) in Quebec City, Canada, over more than 9 years. Of the 11 PAFFs identified, six followed hip arthroplasty, three knee arthroplasties and two occurred in patients with both [38]. Whilst most PAFFs and PFFs following hip arthroplasties were Vancouver B1 fractures (fracture around the stem), PAFFs following knee arthroplasty tended to occur more proximally, away from the prosthesis. Hashimoto et al. prospectively reviewed cases of AFFs (n = 61) and included periprosthetic femoral fractures far from the prosthesis after total knee arthroplasty (TKA) without stem extension and defined them as periprosthetic AFFs (n = 4, 6.6%) [39]. Patients with hip arthroplasty were excluded. Biomechanical analysis using computed tomography (CT)-based finite element analysis (CT-FEA) revealed that the tensile stress distribution in one patient shifted from the distal to the proximal femoral diaphysis after TKA, corresponding to the fracture site. The authors hypothesised that both suppressed bone turnover from anti-resorptive treatment and mechanical stress due to femoral bowing may contribute to PAFF development.
Currently, the lack of a standardised definition hampers accurate estimation of PAFF incidence. Key questions remain: Should PAFFs be defined as occurring only after hip arthroplasty, knee arthroplasty or both? What distance from the prosthesis constitutes a PAFF? Is bisphosphonate exposure essential for diagnosis? Clinicians should be alert to atypical features of PFFs, particularly in patients on long-term anti-resorptive treatment.
Atypical Fractures at non-classical SitesAt present, the ASBMR AFF case definition is limited to fractures located along the femoral diaphysis, originating at the lateral cortex [3]. Increasingly, case reports and case series have reported fractures with features like AFFs occurring at sites distinct from the femur [40] (Fig. 3). We recently published a systematic review of all cases of atypical fractures in patients (aged > 18 years) receiving long-term anti-resorptive therapy (> 3 years) and identified 149 cases of atypical fractures [41]. The ulna, followed by the tibia, were the most frequent fracture sites. All patients were taking anti-resorptive therapy prior to/at the time of fracture, most commonly alendronate. Like the ASBMR AFF case definition, the most common atypical fracture characteristics were the transverse fracture line (95%), non-comminution (98%) and cortical beaking (67%). Fractures at non-classical sites with atypical features should raise suspicion and prompt consideration of anti-resorptive cessation, limited weight bearing and surgical management if appropriate. An update of the ASBMR case definition may be timely.
Fig. 3
Preoperative radiography of bilateral forearm demonstrating left ulnar shaft fracture.
(Courtesy of BMC Musculoskelet Disord).
Update on PathophysiologyGenetic SusceptibilityThe development of AFFs in families, bisphosphonate-naïve individuals and individuals with monogenic bone diseases have raised suspicion of a genetic predisposition underlying AFF development [42,
Comments (0)