Study population
In this prospective longitudinal study, healthy children and adolescents aged 3 to 17 years who participated until adulthood in the ongoing Dortmund Nutritional and Anthropometric Longitudinally Designed (DONALD) study were examined. The DONALD study started as an open cohort in 1985 in Dortmund, Germany, and has since then prospectively collected data on anthropometrics, diet, metabolism, and growth and development from infancy to adulthood in healthy volunteers [11].
After the age of 2 years, yearly examinations of children are performed, including medical anamnesis, dietary recordings, anthropometric measurements, and 24-h urine collections (the latter at or after age 3). Participants older than 18 years are invited to provide a fasting blood sample (typically every 5 years). All evaluations are performed with parental and older children’s written consent. The study protocol was approved by the ethics committee of the University of Bonn, Germany (approval numbers. 098/06 and 185/20) and conducted according to the guidelines of the Declaration of Helsinki.
Participants with a minimum of five eligible 24-h urine collections, i.e., at least two collected within ages 3–8 years and at least three collected during adolescence (ages 9–17 years) were initially considered, resulting in 578 participants. Those participants who had at least five 24-hour urine samples with available measured values of PO4 excretion between ages 3 and 17 years and from whom an adult blood sample was provided were further selected (n = 343). Finally, a total of 159 participants were included in the study, all of whom – between ages 18 and 35 – had collected a 24-h urine sample around the time of the blood sample donation. None of these 159 subjects were using antihypertensives, antihypotensives, beta-blockers, calcium channel blockers, RAAS inhibitors, corticosteroids, or diuretics. Outcomes of interest, i.e., catecholamines, were measured in these adulthood 24-h urine samples.
Anthropometric measurements
Anthropometric measurements were performed by trained nurses following standardized procedures, with participants dressed in underwear and barefoot [12, 13]. Standing height was measured to the nearest 0.1 cm with a digital wall-mounted stadiometer (Harpenden, Holtain Ltd, Crymych, UK), while body weight was determined to the nearest 0.1 kg using an electronic scale (Seca 753E; Seca Weighing and Measuring Systems, Hamburg, Germany). Height and body weight measurements were then used to calculate body mass index (BMI) and body surface area (BSA), according to the formulas: BMI (kg/m²) = weight/height2 and BSA (m²) = 0.007184 x height (cm)0.725 x weight (kg)0.425, as described by Du Bois and Du Bois [14].
Skinfold thickness measurements were conducted bilaterally at the triceps and subscapular, with precision to the nearest 0.1 mm, using a Holtain caliper. Body fat percentage (BF%) was subsequently estimated using the skinfold data and the equations of Slaughter et al. [15]. Fat mass index (FMI) was calculated by dividing fat mass by height squared (kg/m2).
Urinary measurements
Each child and their parents were provided with personal and written instructions on how to collect the 24-h urine sample according to standardized procedures. Urine samples were self-collected at home using Extran-cleaned (Extran, MA03; Merck), preservative-free, 1-L plastic containers. The collected samples were stored at −18 to −20° C until thawed for analysis [16].
Urinary creatinine concentrations were quantified with a creatinine analyzer (Beckman-2; Beckman Instruments, Fullerton, CA, USA), based on the kinetic Jaffé procedure. Samples with daily creatinine excretion levels below 0.1 mmol/kg were excluded from the analysis [17] to reduce potential errors in urine collection. Urinary urea levels were determined using the urease-Berthelot method (Randox Laboratories, Crumlin, UK). Uric acid concentrations (mmol/L) were assessed employing the uricase method using the Uric Acid plus kit (Roche Diagnostics GmbH, Mannheim, Germany) [16].
The alkalizing components of the urinary potential renal acid load (uPRAL), i.e., the mineral cations sodium, potassium, calcium, and magnesium were quantified using flame atomic absorption spectrometry (Perkin Elmer 1100 Spectrometer; Perkin Elmer, Überlingen, Germany). Urinary excretion rates of the anions phosphate, sulfate, and chloride were determined using a Dionex 2000i/SP ion chromatograph containing an ion Pac AS4A column (Dionex GmbH, Idstein, Germany). The uPRAL was calculated according to the formula:
uPRAL = Chloride (mmol/d) + sulfate (mmol/d) x 2 + phosphate (mmol/d) x 1.8 – sodium (mmol/d) – potassium (mmol/d) – magnesium (mmol/d) x 2 – calcium (mmol/d) x 2) [18]. The ion excretion in mmol/d were converted to milliequivalents per day (mEq/d) by multiplying with the respective ionic valence [19].
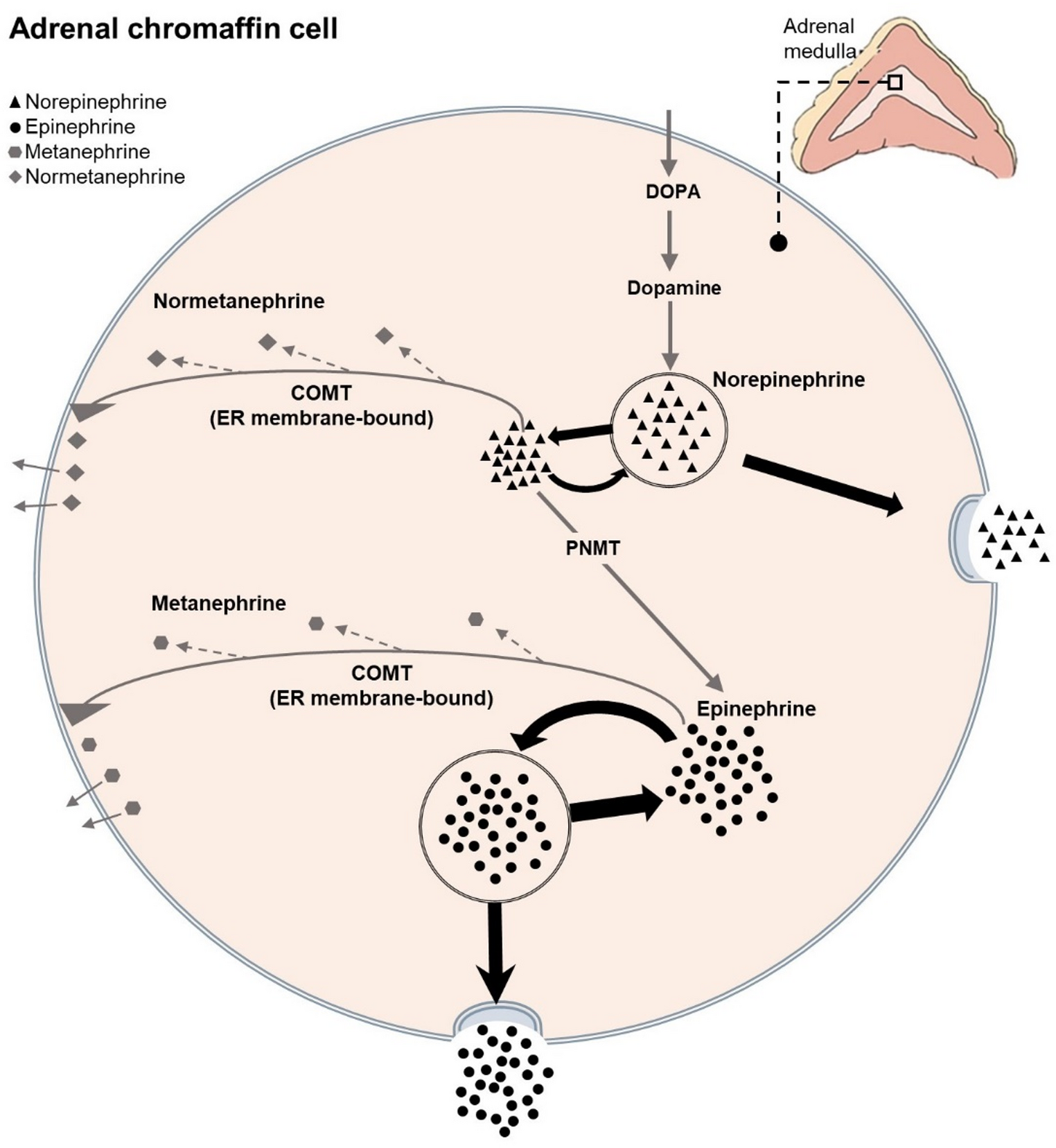
Urinary free catecholamines, i.e., epinephrine, norepinephrine, and their metabolites metanephrine and normetanephrine, were quantified using liquid chromatography-tandem mass spectrometry (LC-MS/MS). Measurements were performed at the Institute of Clinical Chemistry and Laboratory Medicine, Dresden, Germany, based on a method described earlier [20], with minimal changes regarding the mass spectrometric detection system now using a QTRAP 6500+ (Sciex).
Blood measurements
Venous blood samples (< 20 ml) were collected after an overnight fast, centrifuged promptly at 4 °C within 15 min, and stored at −80 °C.
Plasma insulin concentrations were quantified with an immunoradiometric assay (IRMA; DRG Diagnostics, Marburg, Germany) and insulin resistance was evaluated using the homeostasis model assessment (HOMA-IR) [21].
Serum levels of uric acid, urea, glucose, LDL, and HDL cholesterol, as well as plasma concentrations of albumin, creatinine, triglycerides and phosphate were analyzed using a Roche/Hitachi Cobas c311 analyzer (Roche diagnostics, Mannheim, Germany) at the clinic laboratory of the Pediatric Clinic in Dortmund, Germany.
Statistical analysis
All statistical analyses were conducted using SAS statistical software (SAS Institute Inc., Cary, NC, USA; version 9.2), with significance set at p-value < 0.05. The distribution of all variables was examined using the Shapiro-Wilk test and Q-Q plot.
Descriptive data of the participants are presented as means (± SD) for normally distributed variables and as medians (25th, 75th percentiles) for non-normally distributed variables. Differences in phosphate excretion between youth and adulthood assessments were analyzed using a paired t-test for normally distributed data. Furthermore, differences in catecholamine excretion between males and females were tested using an independent t-test, assuming normal distribution of the data. HOMA-IR values were log10 transformed in all regression models to normalize the distribution.
Anthropometric measurements and all pre-adulthood 24-h urinary biomarkers were internally standardized (mean = 0, SD = 1) by sex and age and the standardized deviation scores (SDS) were averaged as means of all individually available measurement points for each participant. The anthropometric and 24-h urinary excretion data from the growth period were then included in the analyses as the respective individual arithmetic means of SDS.
To examine the prospective associations of long-term high phosphorus intake (assessed by PO4 excretion) in childhood and adolescence with the adulthood outcomes—specifically epinephrine, norepinephrine, and their metabolites metanephrine and normetanephrine— multivariable linear regression models were conducted (PROC GLM in SAS). The assumptions for multiple linear regression models, including normal distribution of residuals, linearity, absence of multicollinearity, and homoscedasticity, were tested and not violated. Although diet-by-sex interactions were not observed for any of the catecholamines examined, sex-stratified regressions were conducted to account for the fact that males’ and females’ catecholamine responses have been reported to differ depending on the stressor [22,23,24].
To be included in the final sex-stratified statistical model, each potential covariate was tested separately using stepwise regression and further backward elimination. Covariates were included in the regression model if they modified the association between the exposure variables PO4 excretion and the outcomes epinephrine, norepinephrine, metanephrine or normetanephrine, i.e., if (i) changes in the β coefficient of predictors were ≥ 10%), (ii) they had an independent and significant effect on each outcome (P < 0.05), or (iii) they improved the explained variability of the model. Additionally, the backward elimination method was employed to refine and optimize the model. Variables were retained in the model if they met the predetermined significance level of p = 0.20. Finally, the sex-stratified multilple linear regression models were adjusted for the following covariates: (i) the growth period SDS means of FMI, 24-h urinary urea-nitrogen, urinary creatinine, urinary volume, urinary calcium and urinary potential renal acid load (uPRAL), and (ii) the blood parameters phosphate, creatinine, urea, albumin, uric acid, triglycerides, LDL, HDL glucose and insulin or HOMA-IR.

Comments (0)