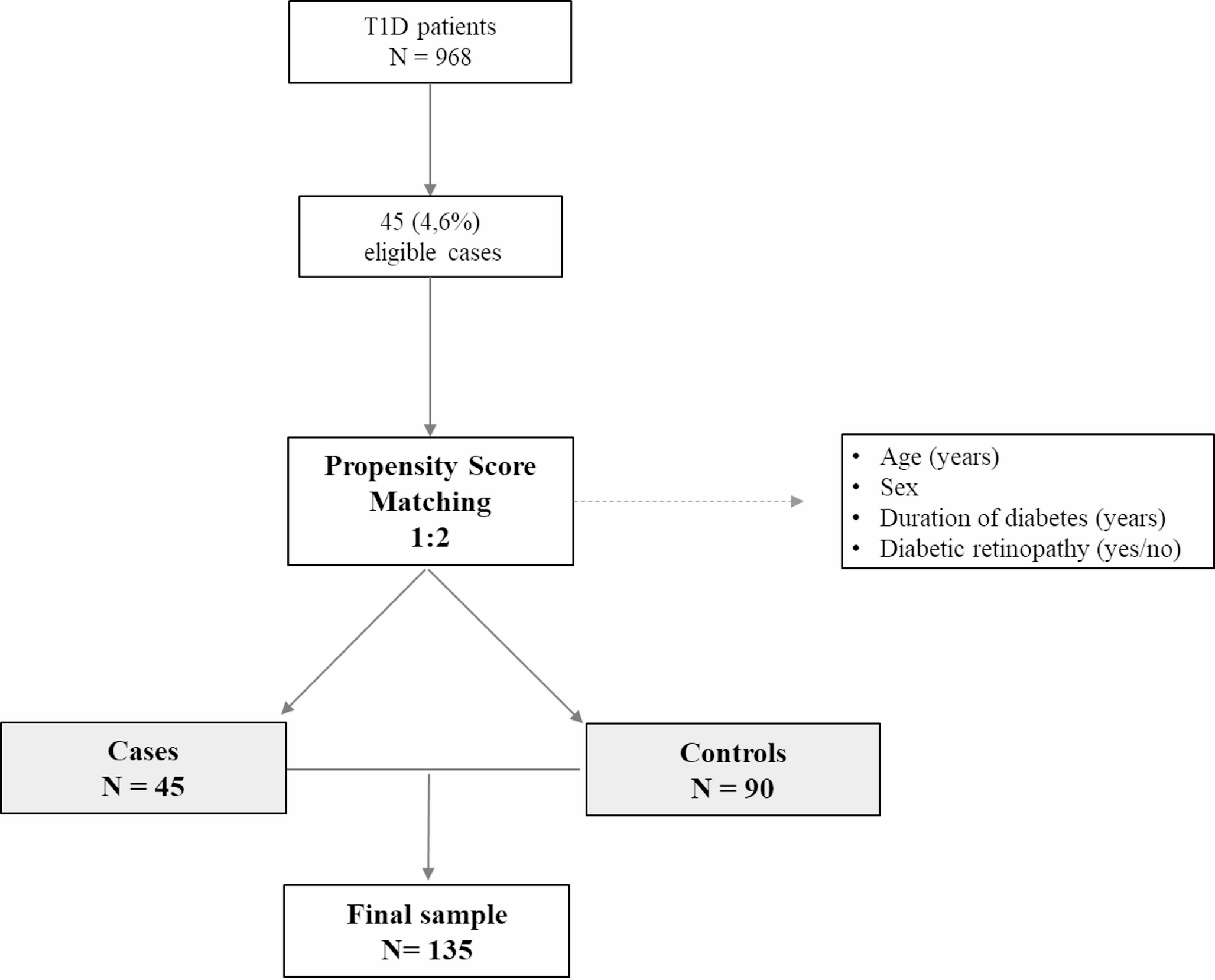
This study is a retrospective case-control analysis conducted at a tertiary care hospital in Spain. Among a cohort of 968 individuals diagnosed with T1D aged over 18 years and actively followed up in the hospital’s dedicated diabetes outpatient services, 45 cases of DH were identified. Each case was matched with two controls based on age, sex, diabetes duration, and the presence of retinopathy, resulting in a final sample of 135 subjects.
Inclusion criteria
For the purposes of our study, the definition of diabetic hand encompassed diagnoses made by specialists in endocrinology, rheumatology, or orthopedics, including at least one of the following conditions: carpal tunnel syndrome, flexor tenosynovitis (“trigger finger”), diabetic cheiroarthropathy, Dupuytren’s contracture, and De Quervain’s tendinitis. Diagnoses were primarily clinical and established using the following criteria:
Dupuytren’s contracture: Presence of nodules or cords at the palmar or digital level, contractures, or skin retraction.
Diabetic cheiroarthropathy (limited joint mobility): Presence of the “prayer sign” (inability to approximate the palmar surfaces of the proximal or metacarpophalangeal joints).
Carpal tunnel syndrome: Pain, numbness, or paresthesia from the thumb to the radial side of the ring finger, with a positive provocative test (Tinel’s and/or Phalen’s signs) or confirmation via electromyography.
Trigger finger: Presence of locking or clicking during finger flexion-extension, along with restricted phalangeal movement.
De Quervain’s tendinitis: Pain over the radial styloid with a positive Finkelstein test.
Cubital nerve compression: Pain, numbness, or paresthesia of the fourth and fifth digits and ulnar aspect of the hand, with a positive provocative test (Tinel’s sign) or confirmation via electromyography.
Exclusion criteria
Individuals under 18 years of age, those with a prior diagnosis of rheumatoid arthritis, osteoarthritis of the hand, or traumatic hand conditions, and individuals with other forms of diabetes mellitus were excluded.
Data collection
The data collected comprised diagnosis and year of diagnosis, coexisting hand pathologies, need for surgical intervention and its timing, and use of corticosteroid injections. Additionally, information on bilaterality and recurrence of hand pathology was recorded. Demographic variables included age, sex, body mass index (BMI, kg/m²), duration of diabetes, and cardiovascular risk factors (smoking, alcohol use, hypertension, dyslipidemia, and the intensity of lipid-lowering therapy per the 2019 ACC/AHA guidelines [11]). The type of diabetes treatment (multiple daily insulin injections or continuous subcutaneous insulin infusion) and the presence of microvascular (retinopathy, nephropathy, or distal symmetric polyneuropathy) and macrovascular complications (presence of ischemic heart disease, acute cerebrovascular events, acute pulmonary edema, peripheral artery disease, and diabetic foot) were also documented. Smoking was defined as consuming at least one cigarette, cigar, or pipe per day (excluding electronic cigarettes), and ex-smokers were defined as those who previously met this criterion but had quit by the time of the study.
Laboratory variables included the mean of the three most recent glycated hemoglobin (HbA1c) values before DH diagnosis (or, for controls, the values closest to the matched case’s diagnosis date), lipid profile (total cholesterol, LDL-C, HDL, and triglycerides), and renal profile (glomerular filtration rate estimated using CKD-EPI and microalbuminuria classified per KDIGO 2024 guidelines [12]). Diabetic retinopathy was categorized based on the International Clinical Diabetic Retinopathy Severity Scale [13] and recorded as present or absent. HbA1c was routinely measured using high-performance liquid chromatography (ADAMS A1c HA8180 V ARKRAY®), and cholesterol was analyzed using enzymatic methods (Alinity C Cholesterol Reagent Kit, Abbott).
Continuous glucose monitoring metrics near the diagnosis of DH were also included, such as average glucose (mg/dL), time in range (70–180 mg/dL), time below range (< 70 mg/dL), time above range (> 180 mg/dL), and glucose variability coefficient.
Statistical analysis
Quantitative variables were expressed as mean and standard deviation if they followed a normal distribution and median and interquartile range if they did not. Normality of continuous variables was assessed using the Shapiro-Wilk test. As all variables followed a normal distribution, results are presented as mean ± standard deviation. Qualitative variables were presented as absolute frequencies and percentages.
To explore the relationship between HbA1c and the presence of diabetic hand, a LOESS curve (locally estimated scatterplot smoothing) was constructed to visually assess the association.
To address the lack of randomization and minimize confounding bias, a propensity score matching method was applied. Cases were matched to two controls using nearest-neighbor matching without replacement. Propensity scores were calculated using logistic regression models, including age, sex, diabetes duration, and retinopathy presence as covariates. This approach resulted in 45 cases matched to 90 controls, comprising a total sample of 135 individuals.
Bivariate differences between cases and controls were conducted using Student’s t-tests or Mann-Whitney U tests for quantitative variables and chi-square tests for categorical variables. For comparisons of normally distributed quantitative variables across multiple categories, ANOVA was used; for non-normal distributions, the Kruskal-Wallis test was applied. A conditional logistic regression model for matched data was developed, adjusting for covariates that were not well-balanced in univariate analyses and that could influence the development of DH.
Statistical analyses were performed using STATA version 17.0 BE-Basic Edition (Lakeway Drive, College Station, TX, USA). A p-value < 0.05 was considered significant.
Ethics
The study protocol was approved by the local Research Ethics Committee and conducted in accordance with the Declaration of Helsinki relating to human studies (Study number 024–5691). The study adhered to the “Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)” guidelines [14].

Comments (0)