
Remember me
With the progression of super-aging, the number of people with dementia continues to rise, making the importance of prevention greater than ever. Large-scale epidemiological studies have demonstrated that hypertension in middle age elevates the future risk of dementia onset, placing hypertension under scrutiny as a modifiable risk factor [1]. The Japanese Society of Hypertension established the “Working Group on Hypertension Management Related to Dementia and Cognitive Impairment Prevention (PCIHM)” within its Academic Committee. This group compiled a review article synthesizing the latest findings from domestic and international basic research. It categorized hypertension-related dementia as “Hypertensive Dementia” and comprehensively outlined its underlying mechanisms [2]. While there is a near consensus that elevated blood pressure in middle age impairs the neurovascular unit through vascular remodeling, atherosclerosis, and endothelial dysfunction, thereby influencing future dementia onset, little consensus exists on whether blood pressure fluctuations in middle age affect cognitive function. For example, den Brok et al. measured visit-by-visit blood pressure variability (BPV) of SBP in 820 participants aged 60-90 years over more than 10 years of follow-up. They found that while changes in BPV at age 90 influenced lifetime dementia risk, no association was seen between high BPV and increased dementia risk between ages 60–80 [3]. They concluded that increased BPV in middle age is not a valid target for dementia prevention. Conversely, Rouch et al. reported that higher systolic BPV was associated with increased dementia risk in 3319 non-hospitalized patients aged 65 years or older [4]. Furthermore, Sible et al. demonstrated, based on autopsy cases, that BPV may promote atherosclerotic and microarteriosclerotic cerebral lesions, potentially leading to cognitive impairment and dementia. They also stated that increased BPV predicted the severity of specific cerebral vascular lesions, including atherosclerosis of the Willis circle and cerebral microarteriosclerosis [5]. Furthermore, Melgarejo et al. conducted a longitudinal study of 24-h blood pressure and cognitive function in 437 participants (mean age 65 years) without dementia. They reported that longitudinal changes in 24-h blood pressure were not associated with cognitive function, but BPV was associated with cognitive decline, with greater nocturnal BPV linked to lower MMSE scores [6]. These findings suggest that BPV may influence dementia onset by increasing vascular load, though the detailed mechanism remained unclear. Results from an animal model examining the relationship between BPV and cognitive function have now been reported [7].
Mendiola et al. created BPV mice by intermittently administering angiotensin II (Ang II) to approximately 1-year-old mice. They demonstrated that 20–25 days of BPV impaired vascular function within the neurovascular complex and induced cognitive decline. Studies using such BPV mice are rare, and the authors state this model was newly developed for this study. Interestingly, the 24-h mean blood pressure in BPV mice was equivalent to that in saline-treated control mice, indicating no hypertension. Thus, the model is described as prehypertensive, concluding that BPV alone strongly contributes to the effects. Thus, it is suggested that chronic BPV, rather than blood pressure levels, targets multiple physiological processes (bradycardia reflex, myogenic response, neurovascular coupling) and represents a risk factor for brain health. A point of note is that while the BPV model can be induced by epinephrine stimulation rather than Ang II, cognitive function has not been examined in the epinephrine model. Ang II itself has been reported to induce impairment of neurovascular unit (NVU), with cerebral vascular damage occurring even at Ang II doses causing only a gradual increase in blood pressure [8]. Recent findings indicate that even in a mouse model of Ang II-induced hypertension lasting only three days, single-cell analysis reveals changes such as endothelial cell damage and impaired function of interneurons. This suggests the possibility that the Ang II-induced NVU impairment observed in the BPV model may also be present here. Therefore, it would be interesting to see if similar cognitive impairments occur in the epinephrine-induced BPV model mice. The association between BPV and cognitive function is an area where findings are increasingly accumulating. Based on the findings from this animal study, it can be said that careful antihypertensive therapy with minimal fluctuations from an early stage is required to prevent cognitive decline in the elderly.
Meanwhile, Schaeffer et al. recently reported results from transcriptomic analysis of the brain in Ang II-induced hypertensive mice using single-cell sequencing [9]. Interestingly, even without elevated blood pressure, three days after Ang II administration showed Ang II signaling-induced vascular endothelial transport impairment and aging, oligodendrocyte differentiation arrest, neuronal functional decline, and network imbalance. Furthermore, by day 42 of Ang II administration, when cognitive impairment became apparent, myelin formation defects, axonal conduction disorders, and progressive neuronal mitochondrial dysfunction were observed. Interestingly, Ang II begins to induce latent impairment of the NVU, causing changes in vascular endothelial cells, oligodendrocytes, neurons, and smooth muscle cells that precede cognitive dysfunction, even before blood pressure elevation is observed. This suggests that by the time blood pressure begins to rise, this impairment may already be progressing.
These two papers of basic research indicate that changes leading to cognitive impairment begin before hypertension becomes overt and that Ang II is the inducing factor. Identifying the influence of Ang II on BPV as a potential trigger and the early burden on the NVU is considered crucial for further elucidating the mechanisms of “hypertensive dementia” (Fig. 1). If useful biomarkers for this purpose can be identified, administering RAS inhibitors even in the absence of high blood pressure might help protect the brain.
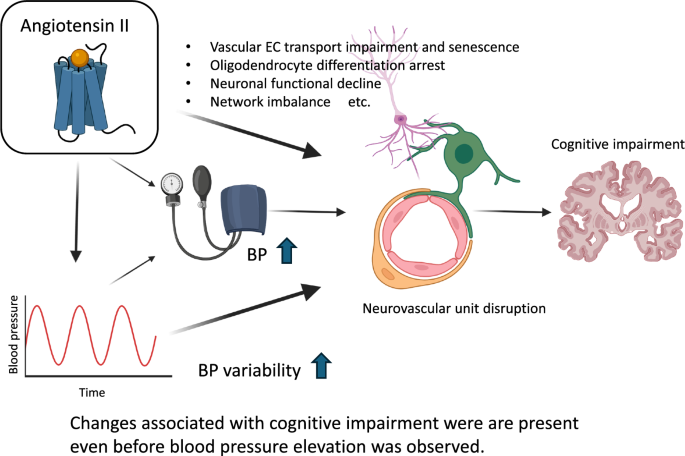
Fig. 1
The possibility of hypertension-related cognitive impairment stemming from brain changes induced prior to the blood pressure elevation caused by angiotensin II (Ang II) administration, as revealed by basic investigations. Increased blood pressure variability due to intermittent Ang II administration induces cognitive decline without elevating the 24-h mean blood pressure. Furthermore, Ang II administration induces damage to cells associated with the neurovascular unit even before blood pressure rises. These findings suggest that in some patients with activated renin-angiotensin system (RAS), hypertension-related cognitive impairment may be induced even in the absence of hypertension, potentially making RAS inhibitors a promising therapeutic target. BP blood pressure, EC endothelial cells
Comments (0)