
Remember me

RFA is a minimally invasive technique for treating lung tumours, particularly early-stage NSCLC, in patients unsuitable for surgery. The procedure uses alternating electrical currents to generate heat, leading to coagulative necrosis in tumour tissue. Due to rapid heat absorption, RFA is particularly effective in well-vascularised areas, ensuring targeted destruction. The integration of RFA with advanced bronchoscopy techniques has expanded its applicability to smaller tumours [10].
RFA is beneficial for patients with early-stage NSCLC or small metastatic nodules, particularly those with comorbidities that increase surgical risk. It preserves lung function, offers shorter recovery times, and has fewer complications than surgical approaches such as lobectomy. Additionally, RFA provides targeted tumour destruction while sparing surrounding healthy tissue [11].
Studies support the safety and efficacy of bronchoscopy-guided RFA. One study reported an 82.6% local control rate in 20 patients treated with cooled-electrode RFA, with no significant complications [10]. Another study documented minimal side effects, such as fever and chest pain, which resolved with conservative management [11]. Bronchoscopic RFA reduces complications, such as pneumothorax, particularly in centrally located tumours near airways. The effectiveness of RFA has improved with the integration of technologies such as electromagnetic navigation (EMN) and robotic-assisted bronchoscopy (RAB), which provide real-time guidance for precise probe placement in peripheral lesions. RAB enhances stability, thereby reducing the risk of probe displacement. Bronchoscopic RFA is a valuable alternative to percutaneous methods, offering shorter recovery times and fewer complications, with many patients discharged within 24 h [11].
Controlling the ablation zone size remains challenging, particularly in complex lung anatomies or tumours adjacent to critical structures. The “heat-sink effect,” caused by the presence of large vascular structures near the target lesion, reduces the effective thermal energy delivered due to continuous blood flow, thereby diminishing RFA efficacy. Future research will focus on improving long-term outcomes and optimising RFA in combination with immunotherapy or chemotherapy. Advances in imaging and navigation technologies will further enhance the precision and efficacy of RFA.
Tumour size is a key determinant of RFA success in treating lung metastases. A study analysing RFA outcomes in patients with pulmonary metastases from various primary malignancies found that recurrence occurred exclusively in tumours larger than 3.5 cm, whereas only 28% of smaller metastases (≤ 3.5 cm) recurred. Additionally, peripheral tumour placement and the absence of large blood vessels (> 3 mm) in proximity were associated with improved outcomes [12].
A systematic review and meta-analysis compared stereotactic body radiation therapy (SBRT) and RFA in patients with inoperable early-stage NSCLC. While short-term overall survival (OS) did not differ significantly between SBRT and RFA at one year (87% vs. 89%, P = 0.07) or two years (71% vs. 69%, P = 0.42), long-term survival was superior with SBRT. The three-year OS rate was 58% for SBRT versus 48% for RFA (P < 0.01), and the five-year OS rate was 39% for SBRT compared to 21% for RFA (P < 0.01), indicating a more favourable long-term prognosis with SBRT.
Beyond survival, SBRT also demonstrated significantly better local tumour control (LC) rates, with a five-year LC rate of 92% compared to 41% for RFA (P < 0.01), suggesting that SBRT is more effective in preventing local recurrence. Treatment-related complications also differed between the two modalities: SBRT was associated with a 9.1% incidence of radiation pneumonitis (Grade ≥ 2), whereas RFA had a 27.2% incidence of pneumothorax. These findings highlight distinct safety profiles and potential post-procedure complications. Given its advantages in survival and tumour control, SBRT may be the preferred modality for patients who can tolerate radiation therapy. However, RFA remains a viable option for select cases with specific risk considerations [13].
Microwave Ablation (MWA)Microwave ablation (MWA) employs electromagnetic waves to generate heat, inducing coagulative necrosis in tumour tissue. Unlike radiofrequency ablation (RFA), MWA achieves higher temperatures more rapidly, enabling larger and more uniform ablation zones. Integrating MWA with advanced navigation systems, such as electromagnetic navigation (EMN) and robotic-assisted bronchoscopy (RAB), enhances precision in targeting peripheral lung lesions. These characteristics make MWA particularly effective for managing early-stage non-small cell lung cancer (NSCLC) and small metastatic nodules. Bronchoscopic delivery further minimises complications, such as pneumothorax and bleeding, which are more common with percutaneous approaches.
A key advantage of MWA over RFA is its efficiency in heating tissue, which translates into shorter procedure times. Unlike RFA, MWA is not significantly influenced by tissue electrical conductivity or increasing electrical impedance within tumour tissue, factors that often limit RFA efficacy. These properties make MWA particularly suitable for larger tumours or cases requiring rapid intervention. Additionally, studies indicate that MWA produces more predictable ablation zones in aerated lung tissue, enhancing its clinical reliability. Preclinical and clinical studies have demonstrated MWA’s safety and efficacy. In a porcine model, bronchoscopic MWA achieved consistent lesion sizes with no significant complications, even in tumours adjacent to blood vessels or airways [14].
The NAVABLATE trial reinforced MWA’s effectiveness in treating peripheral lung nodules, reporting a 100% technical success rate, defined as successful nodule localisation and completion of ablation. The procedure also had a favourable safety profile, with only a 3.3% incidence of mild haemoptysis and no cases of pneumothorax or death. These findings support MWA’s role in managing small, inoperable lung tumours, particularly in patients unsuitable for surgery or stereotactic body radiation therapy (SBRT) [15, 16]. A 2023 multicentre retrospective study further demonstrated MWA’s efficacy and safety in treating ground-glass nodule-like lung cancers. Pneumothorax was the most common adverse event; however, no 30-day mortality was reported [17]. Despite these promising results, larger multicentre trials, including interventional bronchoscopists beyond high-volume centres, are needed to validate safety outcomes in broader clinical settings.
Advancements in imaging and navigation have enhanced the precision of MWA procedures. Platforms such as Illumisite, which integrate real-time fluoroscopy with EMN, improve lesion targeting accuracy while minimising damage to surrounding tissue [18]. However, variability in ablation zone size, particularly in aerated lung tissue, remains a challenge. Retrospective studies have demonstrated that EMN-guided MWA enables precise targeting of lung tumours while preserving adjacent healthy tissue. One study evaluating EMN-guided MWA in early-stage lung cancer reported complete ablation of all targeted nodules, with no disease progression at 12 months [14]. One study evaluating EMN-guided MWA in early-stage lung cancer reported complete ablation of all targeted nodules, with no disease progression at 12 months [19]. Similarly, MWA for ground-glass nodules achieved a 100% success rate with only mild, self-limiting complications [15].
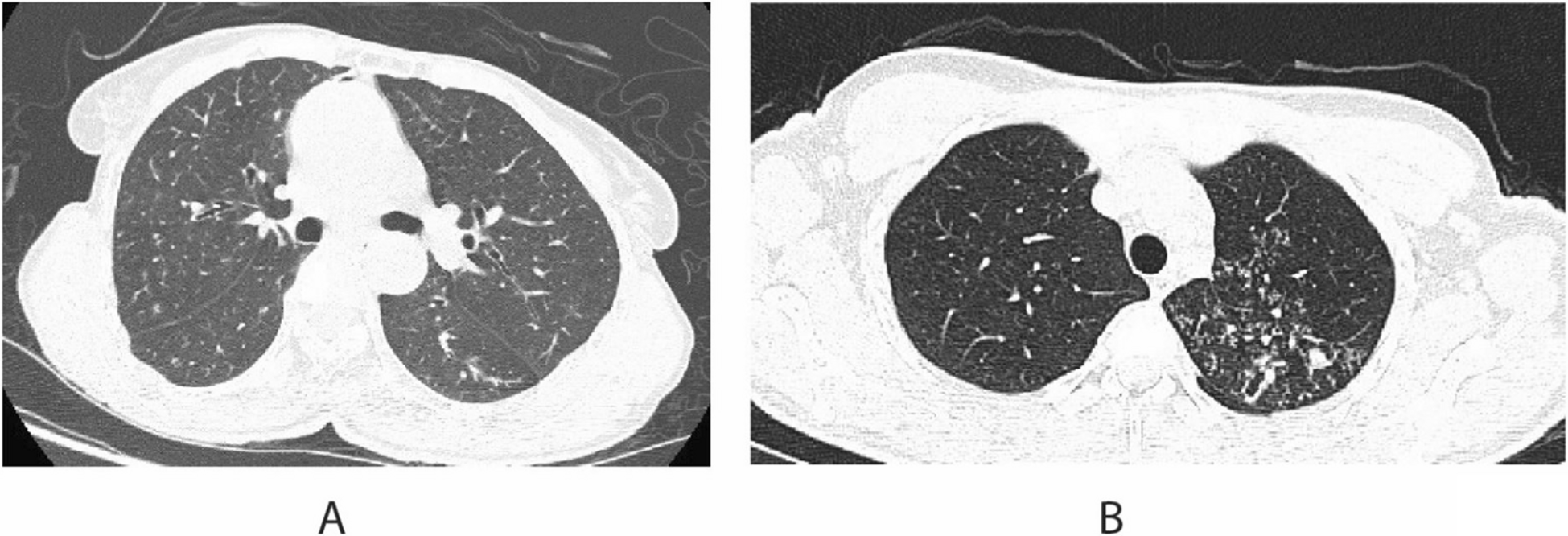
A 2023 meta-analysis comparing stereotactic body radiation therapy (SBRT) and image-guided thermal ablation (IGTA), including MWA and RFA, in inoperable early-stage NSCLC analysed 2,691 IGTA patients and 54,789 SBRT patients. The study found SBRT provided superior local tumour control, with significantly lower 1-year and 2-year local tumour progression rates (OR = 0.2, 95% CI = 0.07–0.63). Among IGTA modalities, MWA showed significantly better disease-free survival (DFS) than RFA at 2 and 3 years (OR = 0.26 and OR = 0.33, respectively), although overall survival rates were comparable [20] (Fig. 1).
Fig. 1
Comparison of thermal diffusion in radiofrequency ablation and microwave ablation. (A) Radiofrequency ablation shows the active ablation zone surrounding the electrode, where tissue destruction occurs through thermal conduction. (B) Microwave ablation demonstrates the active ablation zone surrounding the antenna, with thermal conduction extending further due to electromagnetic energy absorption. Both methods produce a central active ablation zone and a surrounding thermal gradient, but microwave ablation achieves a larger and more uniform thermal diffusion zone compared to radiofrequency ablation. Image created on adobe illustrator
MWA has also been explored for multifocal lung cancer and oligometastatic disease. A 2023 study evaluating ENB-guided transbronchial MWA for multiple lung nodules in 25 patients (56 nodules) reported 100% technical success, with a low complication rate (8% pneumothorax, 4% pleural effusion, pain, or fever) and an average hospital stay of 1.23 days. Ablating multiple nodules in a single session reduced operative and anaesthetic time without increasing complications, suggesting MWA as an efficient, lung-preserving alternative for patients with limited pulmonary reserve, reducing hospital visits and treatment burden [21].
CryoablationCryoablation is a minimally invasive therapy that utilises extreme cold to induce necrosis in tumour tissue. It is particularly suitable for treating centrally located lung tumours, where alternative modalities such as RFA or MWA pose a higher risk of damaging adjacent critical structures, including blood vessels and bronchi. By delivering a freezing agent through a cryoprobe, ice crystals form within cancer cells, leading to cellular destruction [19]. Cryoablation works by freezing the tumour, causing intracellular ice formation that disrupts cellular membranes and induces vascular injury, ultimately leading to cell death. The formation of an "ice ball" extends beyond tumour margins, ensuring comprehensive ablation. This technique is effective for early-stage NSCLC in patients unsuitable for surgery and has shown promise in treating peripheral metastases and recurrent tumours [22].
A key advantage of cryoablation is its ability to treat tumours near sensitive structures without causing thermal injury. The "ice-ball effect" provides margin control, making it particularly useful for complex tumours that are challenging to manage surgically or with heat-based modalities. A study evaluating a thin cryoprobe reported a 100% technical success rate, defined as accurate cryoprobe placement and successful procedure completion, with complete tumour ablation and no significant complications [19]. The integration of robotic-assisted platforms has improved the precision and stability of cryoprobe placement, further enhancing procedural safety and efficacy. However, challenges remain, including variability in tumour response, particularly in larger or complex lesions. Complications such as air leaks and infections can still occur, especially in patients with pre-existing lung disease.
Future advancements will focus on improving procedural accuracy through imaging technologies such as cone-beam computed tomography (CBCT) and autofluorescence (AF). Additionally, combining cryotherapy with immunotherapies, such as PD-1 inhibitors, has demonstrated a synergistic anti-tumour effect, suggesting that this approach may enhance outcomes in patients with advanced or metastatic lung cancer [19, 22, 23] (Fig. 2).
Fig. 2
The intuitive Ion™ robotic-assisted bronchoscopy platform (Model IF1000) (Intuitive Surgical, Inc., Sunnyvale, CA). Key components include: ion system monitor, ion controller, flexible instrument arm, catheter guide, swivel connector, and fully articulating shape-sensing catheter. This platform facilitates navigation and access to peripheral lung lesions for diagnostic and therapeutic transbronchial procedures (Image courtesy of Intuitive Surgical, Inc.)
Irreversible Electroporation (IRE)Irreversible electroporation (IRE), or pulsed electric field (PEF) therapy, is a non-thermal ablation technique that uses electrical pulses to create nanopores in cell membranes, leading to apoptosis. Unlike thermal methods like radiofrequency ablation (RFA) and microwave ablation (MWA), PEF avoids heat damage, making it ideal for tumours near sensitive structures such as blood vessels and airways.
PEF delivers high-voltage pulses that disrupt cellular ion exchange, causing cell death while preserving surrounding healthy tissues. Its precision allows targeting tumours in complex or high-risk areas where thermal techniques pose risks. Although still experimental for lung cancer, early studies show promising results, particularly for tumours located near critical structures where heat-based methods may cause complications [24].
Bronchoscopic Thermal Vapor Ablation (BTVA)Bronchoscopic thermal vapour ablation (BTVA) was first applied to lung cancer treatment in 2021. This technique involves the application of steam to areas of lung parenchyma, with heat adjusted based on the density of the targeted lobe. The resulting inflammatory response leads to lung volume reduction, a method initially approved for treating severe emphysema.
The feasibility and tolerability of BTVA for lung tumours were demonstrated in a 2021 single-arm treat-and-resect clinical feasibility study. Preliminary evidence from this study suggests that BTVA has a high potential for effective tumour ablation [25]. This study involved six NSCLC patients and demonstrated BTVA’s safety and effectiveness. Four patients showed successful ablation, with two achieving near-complete necrosis. Mild chest pain was the only notable side effect, with no severe complications reported. However, vapour back-leakage led to incomplete ablation in some cases, highlighting the need for better vapour delivery control. Additional research is necessary to establish the long-term efficacy and safety of BTVA, particularly for peripheral lung lesions.
Photodynamic Therapy (PDT)Photodynamic therapy (PDT) is a non-invasive treatment that combines a photosensitising agent with light exposure to selectively destroy cancer cells. It is particularly effective for early-stage central airway tumours and serves as a palliative option for inoperable cases [26]. Following systemic administration, the photosensitiser accumulates in tumour cells. Upon activation by a specific wavelength of light, it generates reactive oxygen species, leading to cell death.
A study using a flexible bronchoscope to deliver PDT in patients with endobronchial tumours reported significant symptom improvement, including relief from cough and dyspnoea, with a five-year survival rate of 93% in stage I patients. Bronchoscopic delivery allowed precise light application; however, limitations included the need for multiple treatment sessions and complications such as pulmonary haemorrhage [27]. Another study utilised a composite-type optical fibrescope (COF) inserted via bronchoscopy for peripheral tumours, highlighting the role of bronchoscopy in precise treatment delivery and post-treatment clearance of necrotic tissue [28].
Advancements in flexible bronchoscopes have expanded PDT to peripheral lung tumours, where navigational bronchoscopy ensures accurate interstitial illumination. When combined with surgery, this approach achieved complete tumour ablation, providing a non-invasive treatment option for patients unfit for surgery or radiotherapy. A case of peripheral non-small cell lung cancer (NSCLC) successfully utilised magnetic navigational bronchoscopy for precise PDT fibre placement. Multiple monitored sessions resulted in complete tumour ablation without complications, reinforcing the efficacy of endobronchial PDT for patients ineligible for surgical intervention [29].
The integration of endobronchial ultrasound (EBUS) with PDT has further refined treatment precision. A study employing cylindrical diffuser fibres via EBUS achieved targeted light therapy for airway-obstructing tumours, reducing collateral tissue damage while improving tumour control, particularly in deeper lesions [30]. Lastly, a case report on squamous cell carcinoma demonstrated the use of bronchoscopy in detecting and treating radiologically silent endobronchial lesions. PDT, administered via bronchoscopy after stereotactic body radiation therapy (SBRT), successfully eradicated these lesions [31].
Endobronchial Drug DeliveryApplying inhalable micron- and nanoparticle-based drug delivery systems (DDS) for lung cancer treatment offers a promising approach for localised therapy, reducing systemic side effects. These nanoscale materials enhance bioavailability, lung targeting, and drug stability, with lipid-based nanocarriers, liposomes, and polymer nanoparticles showing potential in preclinical models. While these systems have not yet received clinical approval, they represent a significant advancement in targeted, non-invasive lung cancer therapies [32].
Advancements in brachytherapy have enabled precise endobronchial placement of brachytherapy applicators for peripheral lung tumours using advanced navigation technologies. A study demonstrated a 100% success rate in accurately positioning applicators for patients with non-small cell lung cancer (NSCLC) or metastases, achieving localised treatment with minimal side effects. Previously used primarily for palliative care, this method now shows curative potential for small peripheral tumours, expanding its clinical applications beyond traditional cases [33].
Bronchoscopic intratumoural injections of Endostar (recombinant human endostatin) and cisplatin, combined with chemoradiotherapy, have demonstrated efficacy in treating lung squamous cell carcinoma (LSCC). Endostar, an anti-angiogenic agent that inhibits tumour vascularisation, may enhance chemotherapy effectiveness. A study found that patients receiving these injections had higher remission rates and improved progression-free survival compared to those undergoing chemoradiotherapy alone. This minimally invasive approach, with manageable side effects, presents a potential therapeutic advantage for inoperable LSCC cases [34].
Endobronchial ultrasound (EBUS)-guided intratumoural injections provide another promising strategy for treating NSCLC, particularly in patients with centrally located tumours or those unsuitable for surgery. EBUS allows for precise delivery of chemotherapeutic agents, such as cisplatin, directly into the tumour, maximising local drug concentration while reducing systemic toxicity. This method has shown promise in treating lesions within the bronchial tree, where surgical access is limited, enhancing treatment efficacy while minimising adverse effects [35] (Table 1; Fig. 3).
Table 1 Summary of therapeutic modalities for endobronchial interventionsFig. 3
Mechanisms of energy-based transbronchial interventional techniques (A) Irreversible electroporation applies high-voltage electric pulses to create permanent pores in the cell membrane, inducing cell death without thermal damage. (B) Microwave ablation uses electromagnetic waves to agitate water molecules (H2O), producing heat that spreads via thermal diffusion to destroy tumour tissue. (C) Cryoablation employs argon gas to freeze tissues, causing cellular damage through ice crystal formation and cold diffusion. (D) Radiofrequency ablation generates localised heat using alternating current, leading to tissue destruction through heat diffusion. Image created on adobe illustrator
Other Technologies and TherapiesBronchoscopic laser interstitial thermal therapy has been investigated as a potential ablation method for small peripheral lung tumours. A recent study evaluated the feasibility and safety of diode laser ablation delivered bronchoscopically using a laser delivery fibre (LDF) with a wide aperture. In an ex vivo and in vivo porcine model, optimal parameters were determined to be 25 W for 20 s, resulting in well-defined ablation zones. Computed tomography (CT) at one and three days post-procedure showed progressive cavitation with surrounding consolidation and ground-glass opacity. Necropsy confirmed central char with surrounding necrosis, while histological examination demonstrated well-demarcated zones of tissue injury. The procedure was well tolerated, with only one case of pneumothorax requiring aspiration. These findings suggest that bronchoscopic laser interstitial therapy may be a promising minimally invasive approach for treating early-stage peripheral lung cancer, particularly in medically inoperable patients [57].
Artificial intelligence (AI) is expected to be integrated with robotic bronchoscopy, enhancing real-time decision-making, navigation, and lesion targeting. This integration could improve diagnostic accuracy and procedural outcomes, particularly in early-stage lung cancer [58].
A "one-stop" approach to lung cancer management is also envisioned, where diagnosis, staging, and treatment are combined within a single bronchoscopic procedure. Techniques such as electromagnetic navigation bronchoscopy (EMN), radial endobronchial ultrasound (r-EBUS), and cone-beam computed tomography (CBCT) could be integrated with therapeutic interventions, such as ablation and drug delivery, to streamline patient care and improve clinical outcomes.
Diffusing Alpha-emitters Radiation Therapy (Alpha DaRTs) is a novel technology that utilises radium-244 (Ra-244) to deliver localised alpha radiation for tumour ablation. Alpha particles have short penetration ranges (a few millimetres) but are highly effective at inducing localised cytotoxicity while sparing healthy tissue. In a preclinical study, Alpha DaRTs were precisely implanted in lung and mediastinal tumours using bronchoscopy, ensuring accurate tumour localisation. The devices, designed to be clustered 4 mm apart, allowed alpha particles to diffuse into tumour tissue while preventing unintended exposure to surrounding healthy tissue. The study demonstrated feasibility, safety, and precision, with no significant movement or migration of Alpha DaRTs post-implantation, even in "dirty" lung environments in pigs [59].
Future advancements in ablation therapies may involve combining microwave ablation (MWA) and radiofrequency ablation (RFA) with systemic treatments, such as immunotherapy, to enhance therapeutic efficacy. This combination could be particularly beneficial for patients with early-stage lung cancer who are not candidates for surgery. Additionally, innovations such as water-cooled antennas for MWA and externally cooled electrodes for RFA are expected to improve safety and procedural effectiveness, further expanding the role of ablative therapies in lung cancer treatment [5].
Comments (0)