Risk factor analysis of hypertonic saline non-responders for the treatment of cerebral edema: a retrospective cohort study
Introduction
First line treatment of cerebral edema or elevated intracranial pressure involves hyperosmolar therapy.
Aim
The purpose of this study was to identify risk factors associated with hypertonic saline solutions (HTS) non-responders post HTS bolus for treatment of cerebral edema.
Method
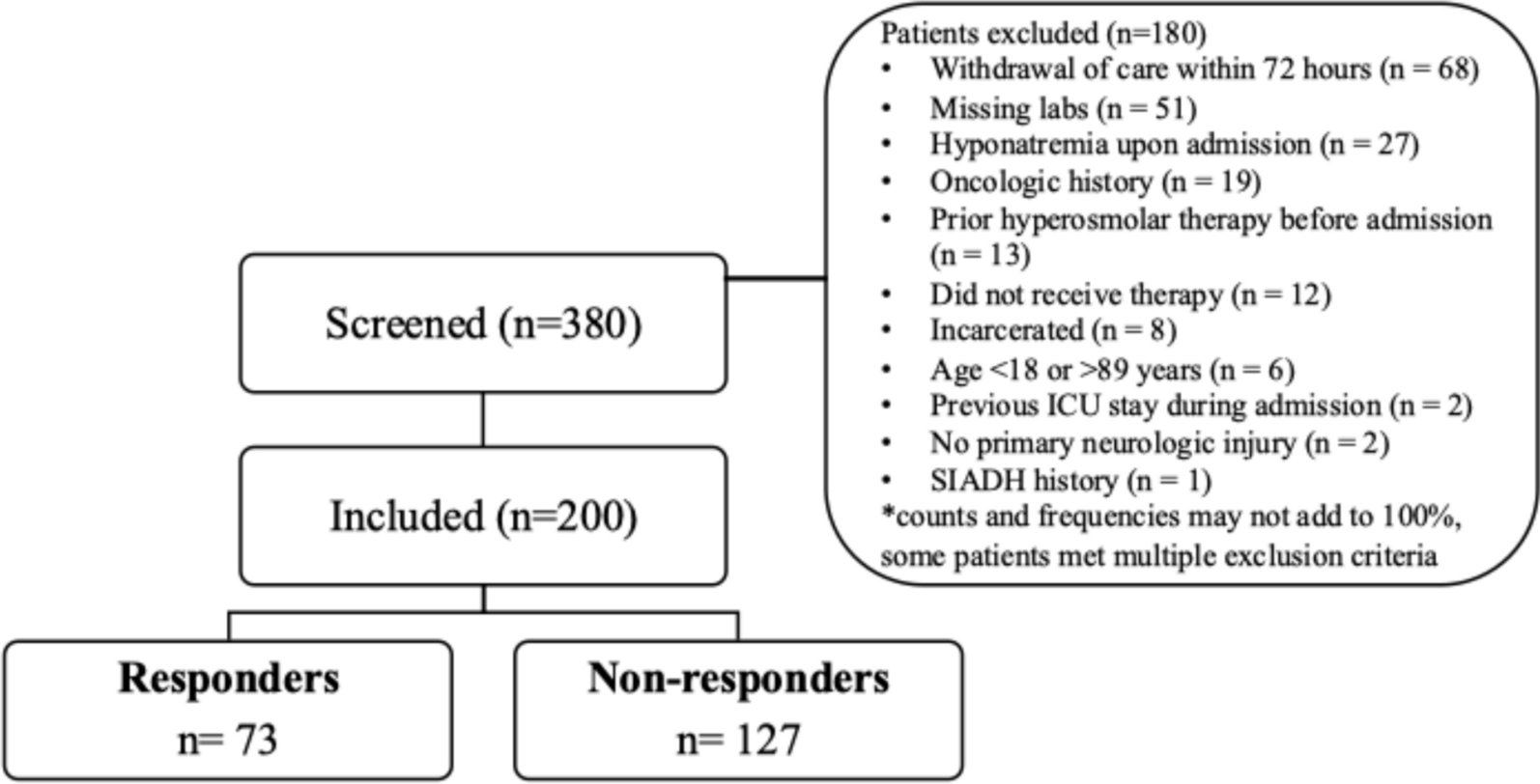
This single center, retrospective cohort study included neurocritical care patients who received one bolus dose of 3% NaCl (> 100 mL) or 23.4% NaCl (30 mL) and obtained one serum sodium level between one and eight hours after administration. The primary outcome was to determine the incidence of HTS non-responders, defined as a serum sodium response of < 5 mEq/L on repeat lab draw, and to identify risk factors associated with HTS non-response (sodium < 5 mEq/L) within 8 h after a HTS bolus dose.
Results
A total of 200 patients were included. The primary neurologic injuries included were acute ischemic stroke (41.5%) and intracerebral hemorrhage (35.5%). For the primary outcome, 127 (63.5%) patients were HTS non-responders. Risk factors associated with HTS non-response, included patients who did not receive mannitol prior to HTS (OR 3.31, 95% CI 1.34–8.17; p = 0.009), male sex (OR 2.43; 95% CI 1.27–4.63; p = 0.007), and patients without intraventricular hemorrhage (IVH) (OR 2.12; 95% CI 1.11–4.06; p = 0.024).
Conclusion
Overall, 63.5% patients were non-responders to HTS. Risk factors for non-response to HTS included no prior mannitol therapy, male sex, and patients without IVH. Further studies are warranted to assess the impact these risk factors have on HTS dosing and the treatment of cerebral edema.

Comments (0)