This study provides, for the first time, a real-life overview of the clinical profile of men seeking consultation for bone health at a tertiary, internationally recognized academic referral Centre for the management of male osteoporosis [18, 24]. In this highly selected cohort, nearly half of the patients were diagnosed with a severe form of osteoporosis, reporting at least one documented osteoporosis-related fracture at the time of the first visit. Consistent with the literature, patients’ medical history revealed a high prevalence of multiple risk factors and comorbidities strongly associated with bone loss [31,32,33]. Despite this, most had never received calcium or vitamin D supplementation, nor bone-active therapy prior to be addressed to a tertiary center. This study also sheds light on referral pathways, providing valuable insights into the real-life workflow related to this still underrecognized disease.
One of the most striking findings is the high prevalence of osteoporosis-related fractures at the initial bone specialist evaluation: 41% of the overall cohort had at least one fracture, with 13.5% presenting with multiple fractures. As expected, fractures rates were highest among elder men (84–89%) but also significantly present in those under 50 years (18–38%) of age. Vertebral fractures were the most frequent (72.7%), particularly at L1 and T12 [34, 35], followed by L2 and T8 [35]. These data support previous observations that the occurrence of an osteoporotic-related fracture leads to bone specialist referral in only a minority of cases—around 4%—and that approximately 40% of men diagnosed with osteoporosis have already sustained one or more fractures by the time of their first visit [15, 31, 36]. Alarmingly, underdiagnosis also persists among hospitalized patients [37]. The relevant percentage of fractures observed in men under 50 represents a novel and important finding, as most existing data focus on older populations [15, 31, 36]. This indicates that men often come to medical attention too late—after fractures have occurred—highlighting a missed opportunity for early intervention to reduce the risk of re-fracturing.
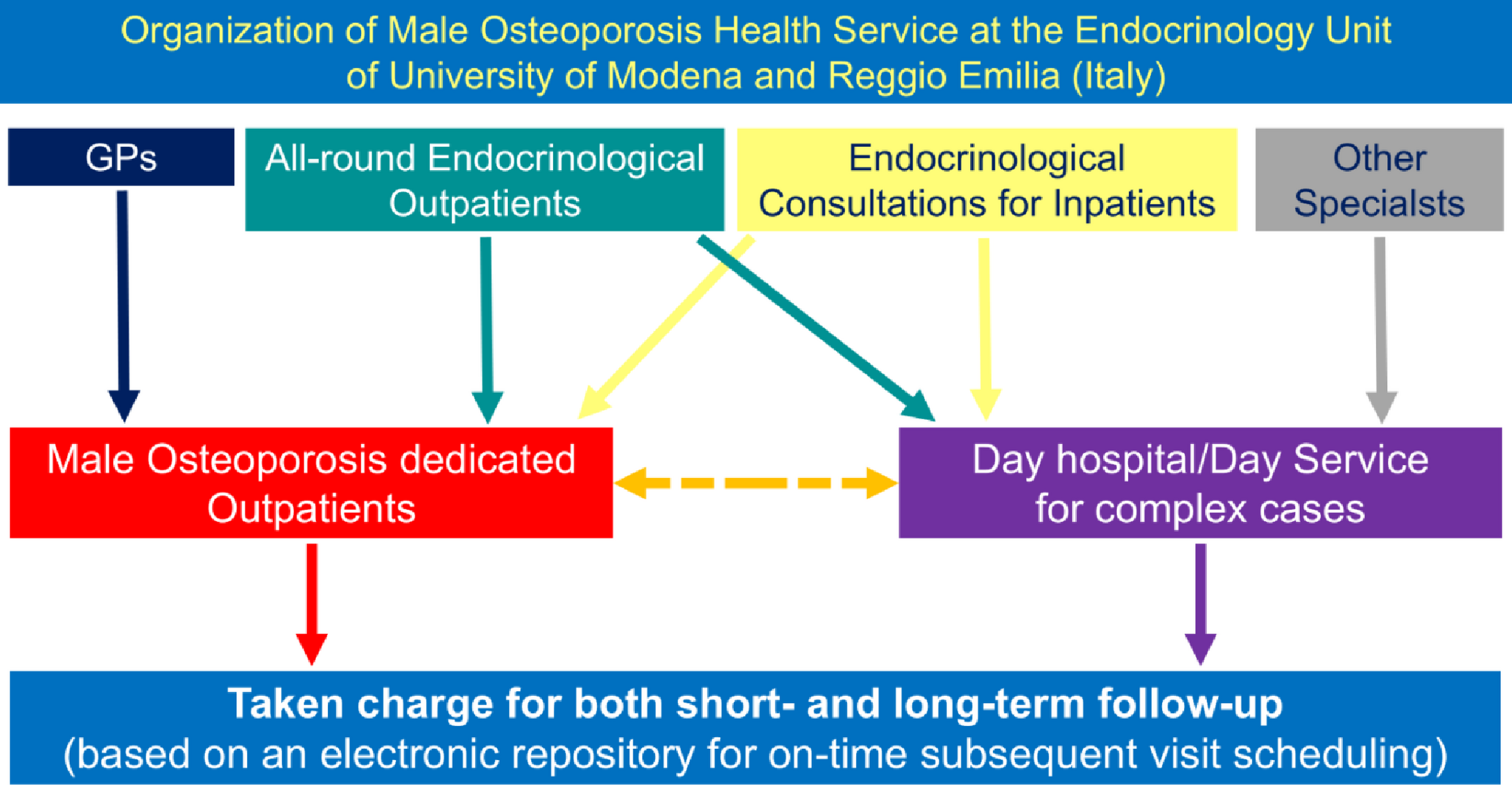
The situation is further worsened by the low rates of calcium/vitamin D supplementation and bone-active therapy in men with fractures and/or low BMD [31, 38]. One in five patients with fractures had never received any form of bone-specific treatment or supplementation. Likewise, only a small proportion of patients undergoing therapies known to promote bone loss—such as corticosteroids or androgen deprivation—were receiving appropriate preventive bone care. This state of affairs needs to be considered in light of the Italian Health Service organization for the management of osteoporosis and of the local implementation in the province of Modena that provides for an initial action of the GP in terms of diagnosis, prevention, and therapy (Fig. 1).
Our findings indicate that patients with fractures were more frequently referred by GP (65.9%) than by specialists (34.1%), suggesting that the initial management pathway often begins in primary care. These data underscore the persistent gap in the recognition and management of osteoporosis in men, particularly in primary healthcare [16, 19, 21], despite this issue having been acknowledged for over two decades [16, 39]. To improve referral pathways, several strategies could be considered. Strengthening communication and collaboration between GP and specialist services may facilitate more timely and appropriate referrals. The development of standardized referral protocols and digital decision-support tools could help ensure that patients are directed to the most suitable level of care. In addition, continuing medical education programs focusing on fracture assessment and referral criteria might enhance practitioners’ confidence and accuracy in identifying cases that require specialist evaluation. Implementing such measures could ultimately optimize patient flow, reduce delays in diagnosis and treatment, and improve overall outcomes for individuals with fractures.
During the first clinical evaluation at our outpatients’ bone clinic, through an accurate medical interview aiming at detecting risk factors/conditions affecting bone, we found that 41% of patients presented with a comorbidity causing osteoporosis, whilst up to 62% was receiving medications inducing bone loss and 54% of fractured patients had never undergone DXA scanning. It is important to emphasize that these data were gathered before any diagnostic testing, based solely on medical history. Therefore, it is reasonable to assume that these percentages would increase if further laboratory or imaging tests were performed, as previously reported [14].
Likewise, laboratory investigations often reveal additional secondary causes of osteoporosis in men, highlighting the critical need for comprehensive diagnostic workups [3, 18, 21]. Yet, most patients had never received such evaluations prior to their visit to a bone specialist in this study. This is further confirmed by FRAX scores, with 43% of patients having a high estimated risk for hip fracture (>3%). While both GPs and endocrinologists generally consider a full osteoporosis workup appropriate in men with high FRAX scores, prior fractures, or chronic corticosteroid or androgen deprivation therapy [40] or presence of diseases causing secondary osteoporosis [41], the proportion of patients actually referred for such assessments remains unacceptably low [38, 42, 43].
DXA findings revealed that the majority of patients over 50 had osteoporosis (42.3%) or osteopenia (44.8%), with only 12.9% showing normal T-scores. Among those under 50, approximately half had abnormal BMD, while the remaining 51.4% had normal values. Clinically relevant is the observation that 17.5% of men with fractures had normal BMD and 26.9% had osteopenia, indicating that DXA alone may not fully capture fracture risk. Hence, bone loss detected by DXA is not the entire problem, but rather part of a syndrome leading to fracture in line with what experts’ opinions emphasize [44]. This supports the concept that bone fragility can exist even in the presence of non-osteoporotic BMD values, particularly in secondary osteoporosis, which is more common in men [15]. The coexistence of osteoporosis-related fractures and normal BMD complicates diagnosis, especially considering the absence of male-specific normative DXA values, which may contribute to false-negative results [18, 21]. These findings emphasize the need for increased awareness of the limitations of DXA and the importance of comprehensive risk assessment. There is a clear need for educational initiatives targeting GPs and specialist physicians, aimed at increasing recognition of male osteoporosis, especially secondary forms. Bone specialists must also take a proactive role in promoting education and research to bridge the persistent knowledge and management gap. In clinical practice, a proper diagnostic work-up—including both laboratory and imaging studies—should be offered to all men at risk for osteoporosis, regardless of age, to uncover potential secondary causes [17, 18, 21]. This approach must extend beyond BMD measurement alone, as secondary osteoporosis and fractures may be present even with normal DXA values.
A major strength of this study is the 14-year observation period and the relatively large sample size, which spans a wide age range, including younger adults. Data on bone health and management were comprehensive, covering key aspects such as comorbidities, fracture history, densitometric measurements, and prior treatments. Many risk factors and lifestyle habits were derived from self-reports and chart reviews, introducing a potential recall and reporting bias. However, unlike many studies relying on electronic health records or ICD coding [14, 15, 45], data in this study were collected directly by clinicians using a uniform clinical approach and centralized documentation system within a structured and dedicated service for male osteoporosis. The main limitations include its retrospective design and potential underestimation of fracture prevalence, as non-clinical fractures may have been missed. Moreover, as the study was conducted in a tertiary care center, the patient population is likely to include individuals with more severe or complex health conditions than those typically managed in primary or community care. This setting may have introduced a selection bias, leading to an overrepresentation of patients with osteoporosis and fragility fractures and, consequently, to higher observed prevalence rates compared with less selected populations. Therefore, caution is warranted when extrapolating these findings to the general population. Nevertheless, the clinic serves a wide geographic area, including referrals from other regions, which enhances the clinical relevance of the results. It also should be noted that the specific organization of the Italian National Service and its structure within the Province of Modena may limit the applicability of these findings to other healthcare settings. Future studies conducted in broader contexts, including primary and community-based care, would be valuable to confirm these observations. Finally, as the study population is predominantly Caucasian (>99%), the findings may not be fully applicable to other racial or ethnic groups.In conclusion, osteoporosis in men presents with a high rate of fragility fractures (about 50%) at the first bone specialist’s consultation in a male cohort referring to a tertiary academic medical Centre. Most had not received appropriate evaluation or treatment beforehand. A comprehensive work-up—including laboratory testing and imaging—should be recommended for all at-risk men, as bone fragility often extends beyond what BMD alone can reveal, especially in case of secondary osteoporosis. These findings underscore the urgent need to raise awareness of male osteoporosis, especially in primary care. Educational initiatives for both physicians and patients are essential, along with greater research efforts to address existing diagnostic and therapeutic gaps.


Comments (0)