
Remember me


The resulting classification performance is summarized in Table 1. This reflects the gross classification of each FFPE block as malignant (FTC) or benign (FA), rather than the detection of individual invasive features or subclassification of FTC. X3DVH achieved a sensitivity of 85.9%, specificity of 100%, accuracy of 89.2%, positive predictive value (PPV) of 100%, and negative predictive value (NPV) of 68.9%.
These findings demonstrate that X3DVH exhibits high specificity. Practically, this implies that when a block is classified as malignant by X3DVH, it is almost certainly malignant, consistent with the PPV observed in this cohort. However, the method failed to identify 14 blocks as FTC that were confirmed by histological analysis, resulting in reduced sensitivity and a lower NPV. Therefore, a benign classification by X3DVH cannot reliably exclude malignancy, and histological confirmation remains essential to establish benign status. Furthermore, even in blocks accurately classified as malignant, histology remains indispensable for confirmation of foci of invasion. The reduced sensitivity of X3DVH is attributable to its lower resolution and contrast relative to conventional histology, reflecting a trade-off for the acquisition of volumetric data. Given the method’s high specificity, its performance in cases misclassified by conventional histology warrants investigation, as the added volumetric information may offer diagnostic utility.
Case StudiesFollowing the validation analysis, X3DVH was applied to five challenging cases in which conventional histology had led to misclassification. These comprised five tumors initially diagnosed as FA but later relapsed (R1–R5), with details of the initial diagnosis and relapse site summarized in Table 2. This cohort provided an opportunity to test X3DVH in clinically relevant scenarios where volumetric information could complement standard histology.
Table 3 provides an overview of the case study results. Cases are categorized according to the presence or absence of VI, while CI was not considered for classification because of its lesser importance and perfect prognosis. In three cases (R1, R2, and R5), X3DVH successfully identified at least one VI, which was subsequently confirmed by targeted serial sectioning. In R4, the diagnosis was revised to UMP, while R3 no additional invasive features were detected. R3 is undersampled in terms of tumor capsule embeddings with 4 blocks prepared for a 6 cm diameter tumor. Thus, invasive features could have been missed during tumor capsule embedding. Except for R3, X3DVH contributed to revising or refining the initial diagnosis of cases that had been misclassified as adenomas.
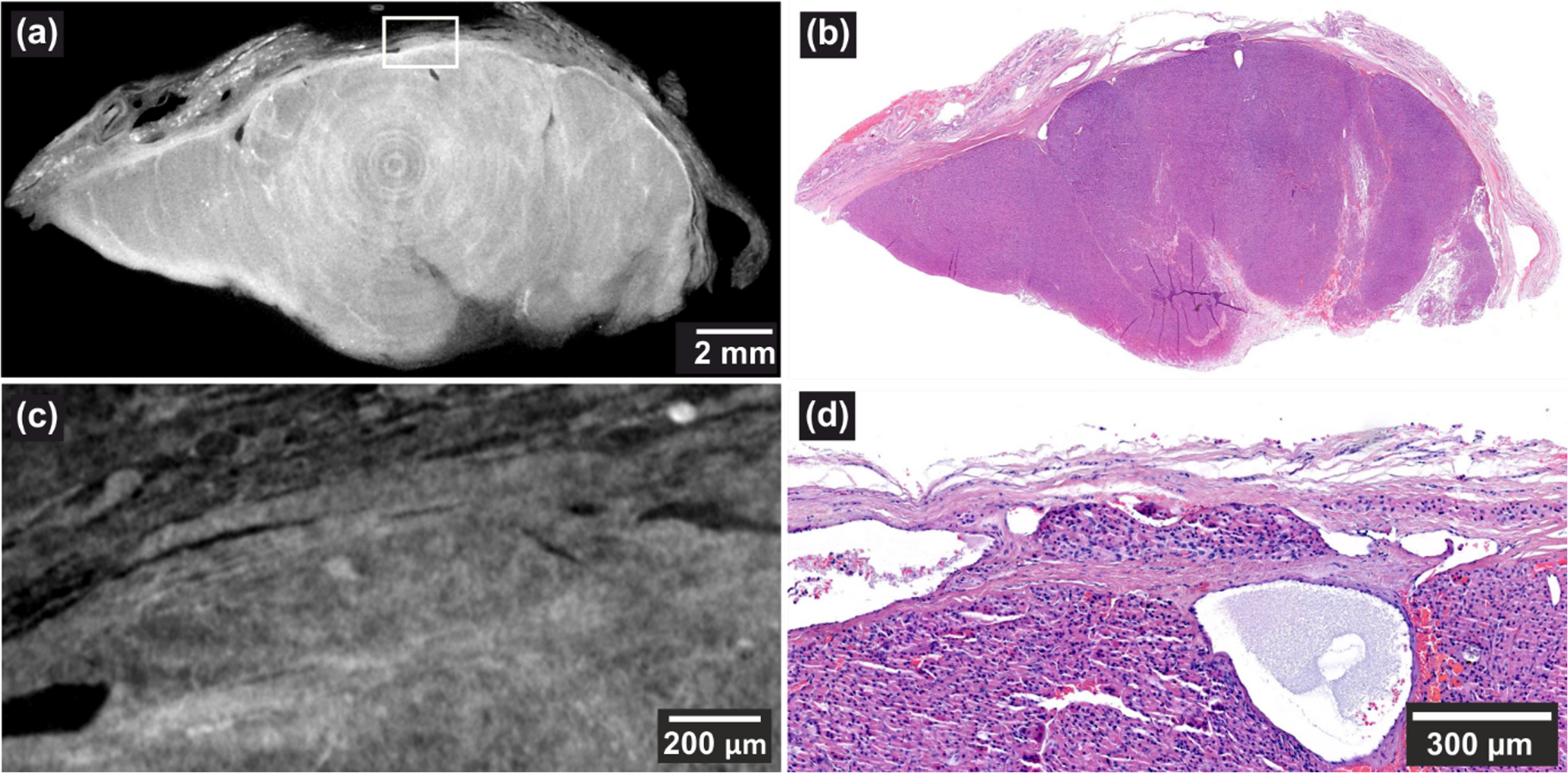
Table 3 Summary of cases assessed by X3DVH and histology. The number of VI sites is listed under the columns “X3DVH” highlighting features detected by 3D virtual histology and under “Histology,” the ones subsequently confirmed or refuted by targeted serial sectioning. The table reports the number of FFPE blocks containing tumor capsule, indicating the extent of tissue sampling relative to tumor diameter, with the number scanned by X3DVH shown in parenthesesR1This case concerns a 66-year-old male who underwent thyroidectomy in 2010. In 2019, the patient experienced rise in Tg level of 2500 ng/mL and retrosternal nodule was found, consistent with encapsulated angioinvasive OTC. This relapse indicates that the original lesion must have harbored malignant features that went unrecognized at the time of the initial diagnosis. Following histological reexamination of nine FFPE blocks from the primary tumor capsule, which showed no suspicious features, the specimen was subsequently submitted for X3DVH screening according to the study protocol. Three regions within a single block were identified as suspicious for VI, with one confirmed as a definite VI. As illustrated in Fig. 1, the VI was located approximately 800 μm deep in the block and was initially detected through a whole-block scan (voxel size = 13.90 μm), shown in (a). A high-resolution local scan at a 3.00 μm voxel size shown in (c), provided enhanced visualization, while high-magnification H&E in (d) confirmed the presence of VI. Several dilated vessels were also observed in the vicinity, further supporting the diagnosis.
Fig. 1
(a, voxel size: 13.90 μm) VI detected ~ 800 μm deep in the FFPE block using X3DVH. (b) Corresponding H&E section shown. (c), voxel size: 3.00 μm) A high-resolution local scan, and (d), depth: ~1360 μm) matching high-magnification H&E image confirm the finding
Of the remaining two suspicious invasion foci, one was identified as a septum, while the other was located at the edge of the tissue and was partially cut off during sectioning. According to WHO classification guidelines, these findings would lead to a revised diagnosis of encapsulated angioinvasive FTC.
R2This case involves a 69-year-old female who was diagnosed with right-sided oncocytic FA in 2017. In late 2023, right-sided cervical nodule was detected, and FNA in March 2024 revealed tumor cells consistent with thyroid oncocytic follicular neoplasm. A right lateral neck dissection was subsequently carried out in April 2024, followed by lung segment resection of metastatic focus, again histologically confirmed as oncocytic differentiated carcinoma, consistent with thyroid carcinoma metastasis.
For the study purpose, five FFPE blocks from the primary 4 cm tumor were examined by X3DVH. While the topmost slice of the FFPE block appeared non-invasive, deeper levels revealed a capsular irregularity measuring approximately 4 mm in diameter, which was located approximately 800 μm deep in the tissue (Fig. 2(a)). However, no clear VI pattern was initially identified. Given that this was the only morphological abnormality seen, targeted serial sectioning was performed. Deeper sections confirmed the presence of VI, as illustrated in Fig. 2(c) H&E and (d) EVG images.
Fig. 2
(a, voxel size: 12.7 μm) VI identified ~ 800 μm deep in the FFPE block, and (b) the corresponding H&E section at the same depth, with high-magnification detail in (c) and the corresponding EVG stain in (d)
R3This case concerns a 42-year-old female who underwent right-sided hemithyroidectomy in June 2016. Notably, for a 6 cm dominant tumor within a goiter, only four blocks were sampled from the tumor periphery, suggesting the absence of grossly suspicious features. In 2024, the patient presented with a bone lesion, and a core biopsy revealed a Tg-positive follicular neoplasia, suggestive of metastatic thyroid-origin disease. A subsequent complementing hemithyroidectomy of the left lobe in August 2024 also resulted in a diagnosis of FA. Although no definitive malignant features were identified in either thyroid lobe, and no ovarian mass was present as a potential alternative source of a primary (i.e., malignant struma ovarii), the presence of distant metastases raises the possibility that carcinoma may have been missed in the 6 cm thyroid nodule.
Upon histological review, no suspicious areas of invasion were identified. X3DVH analysis of the initially resected lobe identified two adjacent regions, approximately 3.5 mm apart that were suspicious for VI (see Fig. 3(a) and (c)). However, serial histological sectioning and review determined both foci to be borderline or equivocal, potentially intracapsular, but lacking definitive evidence of vascular wall penetration (Fig. 3(b) and (d)). Notably, these ambiguous regions were located near the FFPE block cutting plane, an area prone to mechanical deformation and artifact-induced variability. Additionally, the presence of inflammation and inward capsule deflection toward the tumor center raises concerns about a possible histologic alteration following fine-needle aspiration of the thyroid. This phenomenon is encompassed by the term WHAFFT (Worrisome Histologic Alterations Following Fine-Needle Aspiration of the Thyroid), which refers to a spectrum of reactive changes such as pseudoinvasion of the tumor capsule and infarct-like necrosis that can mimic malignancy in thyroid tissue following FNA [19].
Fig. 3
(a, voxel size: 4.6 μm) A suspected VI by X3DVH, which proved to be a false positive by histological inspection in (b). The second suspected invasion is shown in (c), voxel size: 4.9 μm), and its corresponding H&E image in (d), also negative for invasion
R4This case concerns a 54-year-old female patient diagnosed with FA in 2012. A decade later, in 2022, the patient experienced a relapse, with Tg levels rising above 300 ng/mL and small pulmonary foci detected, raising suspicion for metastatic disease. On October 13, 2022, three locally recurrent nodules were surgically resected.
No suspicious areas of invasion were observed on histological re-examination. X3DVH screening was conducted on seven FFPE blocks of the primary tumor. One block revealed a narrow capsular interruption approximately 500 μm below the surface, raising concern for VI, as shown in Fig. 4(a). Targeted serial sectioning and.
Fig. 4
(a, voxel size: 3.7 μm) The capsule irregularity was observed in X3DVH image at approximately 500 μm deep in the blocks, its corresponding H&E image is shown in (b)
corresponding H&E staining of this region confirmed the same focal discontinuity of the capsule (Fig. 4(b)). The capsule appeared split with a rare morphology that may be confounded by surrounding inflammation. Although suspicious, this alteration lacked definitive features of VI and CI. Based on these findings, the lesion was classified as a UMP. The atypical capsular configuration may reflect WHAFFT.
R5This case involves a 67-year-old male who was diagnosed with FA in 2011 after hemithyroidectomy. In 2023, he experienced a relapse, with the recurrent lesion diagnosed as a widely invasive OTC measuring 14.5 cm, confirmed to have VI sites and staged as pT3. The stark contrast between the initial benign diagnosis and the aggressive recurrence highlights the potential for histologically indolent-appearing lesions to undergo malignant progression over time.
Nine FFPE blocks encompassing the tumor-capsule interface were examined. Histological revision revealed no evidence of invasive foci. X3DVH promptly identified two discrete foci of CI in separate blocks. However, histological assessment of the primary tumor was complicated by artifacts from mechanical sectioning, including tumor fragmentation and contour distortion, particularly due to the presence of a thin, hemorrhagic capsule. Therefore, the suspected features were discarded as artifacts. In a second block, X3DVH suggested a possible VI presented in Fig. 5(a) region of interest (ROI 1). While serial sections revealed that this putative VI was artifactual, resulting from an irregularly thickened vessel wall (Fig. 5(c)). Through serial sectioning multiple small caliber VI sites were revealed that could not be resolved by X3DVH (Fig. 5(a) ROI 2).
Fig. 5
(a, voxel size: 22.3 μm) X3DVH scan showing a suspicious but histologically refuted VI (ROI 1) and a VI that was discovered by serial sectioning in (ROI 2). The corresponding H&E section at ~ 450 μm depth is shown in (b). ROI 1 was discarded histologically (c), while ROI 2 confirmed a true VI (d)
The histological image is shown in Fig. 5(e). Histologically identified VI in Fig. 5(b) was discovered in the vicinity of ROI 1 which is shown in high magnification in Fig. 5(e). The presence of multiple VIs clarifies the biological basis of the patient’s tumor relapse. This VI should be in the resolution limit of X3DVH, but because of the short scan time dedicated to the sample, it was missed.
Comments (0)