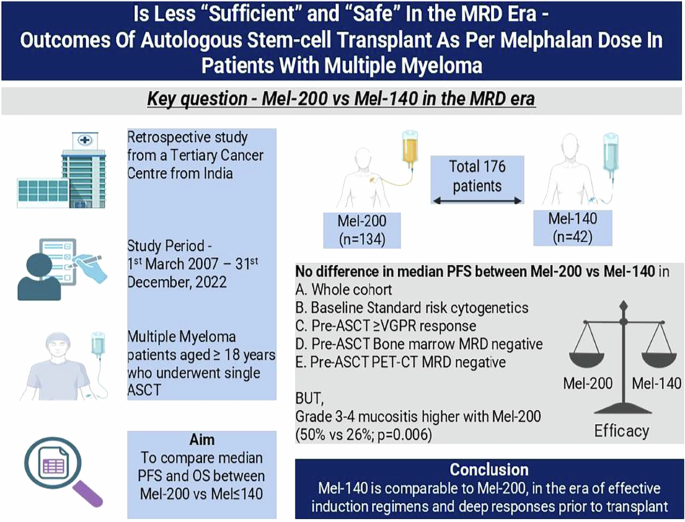
This was a retrospective single-centre study from India, which included MM patients who underwent ASCT over the last 15 years. Our primary objective was to compare median PFS and OS in patients who received Melphalan 200 mg/m2 (Mel-200) versus those who received ≤140 mg/m2 (Mel-140). Our secondary objectives were to compare median PFS in Mel-200 vs Mel-140 for following subgroups: ≥VGPR pre-ASCT, those who underwent ASCT in first-remission, baseline cytogenetics (standard and high-risk), pre-ASCT bone-marrow (BM) flow-cytometry MRD status (Negative and positive), and 18-FDG-PET-CT status prior to ASCT (Negative and positive).
Between 1st March 2007–31st December, 2022, 178 patients underwent 192 ASCTs. Amongst these 178 patients, two patients with tandem transplants and patients who underwent second transplant at relapse were excluded (due to higher cumulative melphalan dose). Thus, we analysed 176 ASCTs in 176 patients (Supplementary Fig. 1). All methods were performed in accordance with the relevant guidelines and regulations. This study was approved by our Institutional Ethics Committee (IEC-III) [Project number 901182 approved on 09 August 2025]. Informed consent was obtained from all participants.
Pre-ASCT work-up included – Hemogram, renal and liver function tests, nutritional status (ferritin, B12, folate levels, transferrin saturation), virology (HIV, HBsAg, anti-HCV, Anti-HBc IgM and IgG, Anti-HBs), DTPA-GFR, MUGA scan for cardiac ejection fraction (EF) and pulmonary function tests (PFT) with diffusion capacity for carbon monoxide (DLCo). In view of literature of higher TRM (6%) in patients with renal impairment [9] and IMWG consensus guidelines for renal impairment [10], we used a GFR cut-off of 60 ml/minute for Melphalan dose-reduction to 140 mg/m2. Apart from GFR, patients with borderline organ functions: EF 40–50%, and/or impaired PFTs (FEV1 or FEV1/FVC ratio <70% or corrected DLCo<65%) received Melphalan doses ≤140 mg/m2, as per discretion of transplant physician.
We reported in ASH-2014 (Abstract#731) that pre-ASCT PET positivity predicted early relapse. Consequent to this, we mandated our institutional policy to do 18-FDG-PET-CT for all patients of MM pre-transplant. Results of pre-transplant PET-CT were considered as either negative or positive, as per IMWG 2016 criteria [11].
BM-MRD was evaluated using a highly-sensitive 13-colour flow-cytometry (sensitivity-0.0001% or 10−6) method, as described before [12]. From 2016 onwards, all our patients underwent BM-MRD pre-transplant as part of institution policy. For analysis, BM-MRD at a threshold of <0.001% or <10−5 was considered negative, while ≥0.001% or 10−5 was defined as MRD positive.
Stem-cell mobilization, maintenance post-ASCT and response monitoring, were as described before [1, 13]. In absence of BM examination pre-ASCT, maximum response was graded as VGPR [11]. For analysis, patients with pre-induction serum creatinine >2 mg/dl were considered as those with baseline renal dysfunction (RD). For stratification as per cytogenetics [mSMART3.0], patients with any one of the following cytogenetics: t(4;14), t(14;16), t(14;20), chromosome-1 abnormalities (1q gain or amplification, 1p deletion) and deletion 17p were considered high-risk [2]. Rest was considered as standard-risk.
An additional matched-pair analysis was done (4:1 ratio for Mel200:Mel140 with a caliper-size of 0.2). This analysis was done using a propensity score from logistic regression with a probit-link function. The score was estimated by adjusting age, ISS-stage, type-of-induction, lines-of-treatment, disease status pre-ASCT and time from diagnosis-to-ASCT (in months). Data was updated till 30th November, 2024. Survival and follow-up were calculated from date of ASCT. Data was tabulated in a Microsoft excel-sheet and analysed using spssv23.0. For categorical variables and numerical data analysis, Chi-square test and Mann-Whitney test were used respectively. Survival was calculated using Kaplan–Meier method and compared using Log-rank test. Subgroup analysis was reported using Forest-Plot. Reported p-values were two-sided and p < 0.05 was considered statistically significant.

Comments (0)