
Remember me


Background: In the DETERMINATION phase 3 trial, relative PFS with RVd–alone vs RVd+ASCT differed between White (n = 540/722, 74.8%; median 44.3 vs 67.2 months; hazard ratio [HR] 1.67, 95%CI 1.29–2.15) and African American (AA) patients (n = 132/722, 18.3%; median not reached [NR] vs 61.4 months; HR 1.07, 95%CI 0.61–1.89). Given that access to care was enhanced in DETERMINATION and race is a social construct, a pathobiological explanation was sought; high prevalence of Duffy null phenotype among AA patients and its known impact on the inflammasome was proposed as an alternative hypothesis for the observed differential treatment effect by race.
Methods: Genomics analysis of baseline peripheral blood samples for SNP rs2814778 classified patients as C/C (Duffy null) or non–C/C (Duffy non–null). Duffy status is currently available for 295 patients (40.9% of intent–to–treat [ITT] population). This cohort is broadly representative but contains fewer AA patients, patients with ECOG PS > 0, and patients with elevated LDH; additionally, treatment duration was longer than the ITT population. Impact of Duffy status on PFS was evaluated with Cox proportional hazards regression in univariate and multivariable models. Heterogeneity of treatment effect was assessed by a test for interaction.
Results: Of 295 patients, 37 (12.5%) were AA, of whom 27 (73.0%) were Duffy null; 256 (86.8%) were White/other race, of whom 1 (0.4%) was Duffy null (Table 1). In all patients in our cohort, PFS with RVd–alone vs RVd+ASCT (median 52.2 vs 82.3 months; HR 1.41, 95%CI 1.01–1.96) was consistent with the ITT population; PFS data in AA patients (median NR vs NR; HR 0.76, 95%CI 0.23–2.50) and White/other race patients (median 49.4 vs 66.5 months; HR 1.52, 95%CI 1.06–2.17) (interaction p–value 0.130) were similar to ITT findings in AA and White patients. PFS (pooled across treatment) was similar in Duffy null vs Duffy non–null patients (12/29 vs 132/266 events/patients; median NR vs 61.9 months; HR 0.78, 95%CI 0.43–1.41). PFS with RVd–alone vs RVd+ASCT was substantially different in Duffy null patients (2/13 vs 10/16 events/patients; median NR vs 44.0 months; HR 0.21, 95%CI 0.04–1.02) compared to Duffy non–null patients (73/121 vs 59/145 events/patients; median 48.4 months vs NR; HR 1.73, 95%CI 1.21–2.46) (interaction p–value 0.002). On multivariable analysis, PFS was significantly longer in Duffy null vs Duffy non–null patients with RVd–alone (HR 0.15, 95%CI 0.04–0.63), but PFS HR was 1.69 (95%CI 0.85–3.37) with RVd+ASCT (Figure).
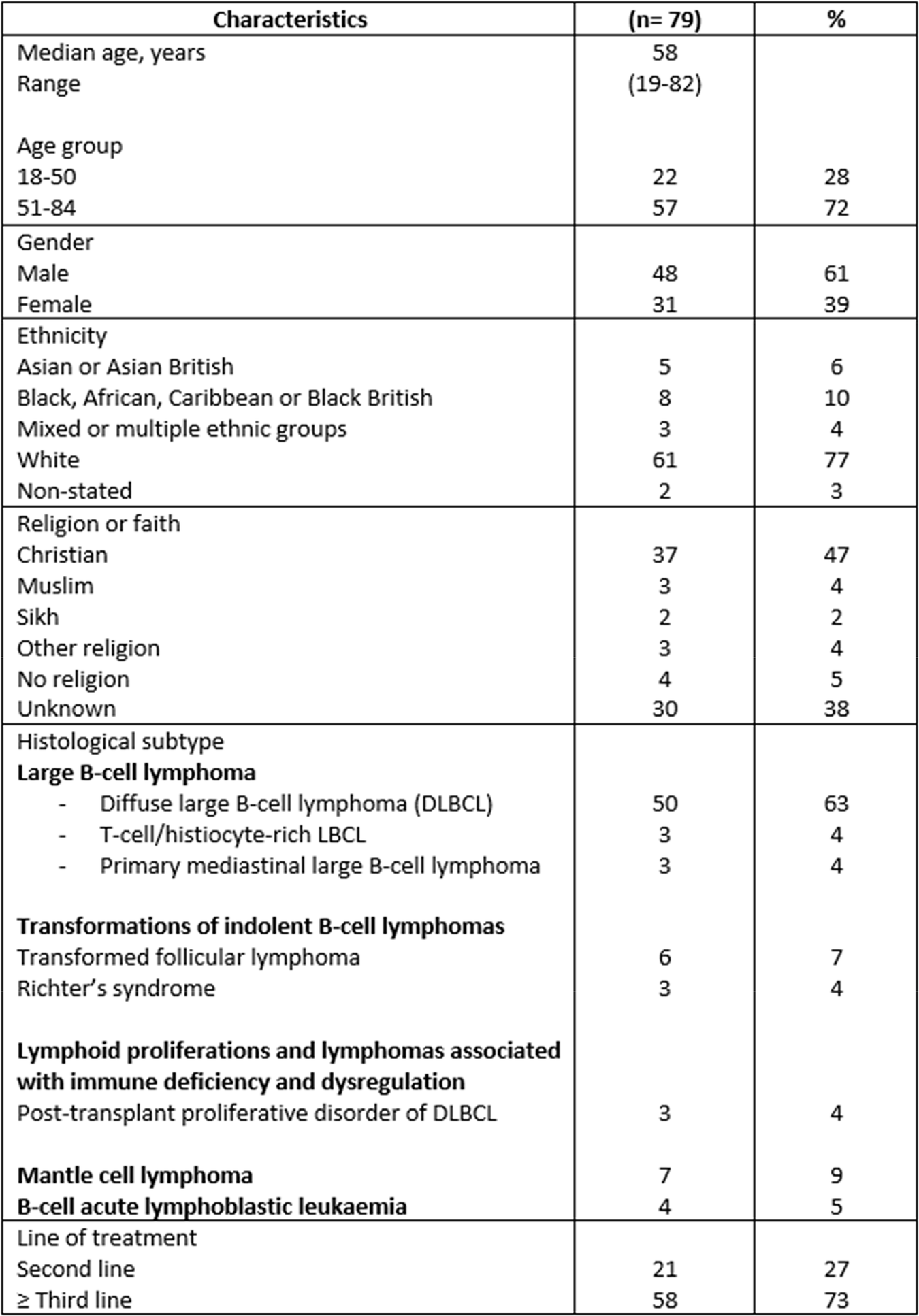
Baseline patient and disease characteristics by Duffy status were assessed for imbalances
RVd–alone, n = 134
RVd+ASCT, n = 161
All, N = 295
Characteristic
Duffy null, n = 13 (9.7%)
Duffy non–null, n = 121 (90.3%)
Duffy null, n = 16 (9.9%)
Duffy non–null, n = 145 (90.1%)
Duffy null, n = 29 (9.8%)
Duffy non–null, n = 266 (90.2%)
Median age, y
55.0
56.0
58.5
54.0
57.0
55.0
Age ≥60 y,%
15.4
35.5
43.8
26.2
31.0
30.5
Male,%
15.4
60.3
68.8
55.9
44.8
57.9
AA / White, other,%
92.3 / 7.7
2.5 / 97.5
100 / 0 (n = 15)
4.9 / 95.1 (n = 144)
96.4 / 3.6 (n = 28)
3.8 / 96.2 (n = 265)
ECOG PS > 0,%
46.2
54.5
37.5
45.5
41.4
49.6
BMI ≥ 30 kg/m2,%
53.8
34.7
43.8
37.9
48.3
36.5
ISS I / II / III,%
53.8/38.5/7.7
47.9/29.8/16.5
50.0/37.5/12.5
49.0/37.2/13.8
51.7/37.9/10.3
48.5/36.5/15.0
LDH > ULN,%
15.4
16.5
37.5
15.2
27.6
15.8
HR cytogenetics,%
25.0 (n = 12)
21.2 (n = 113)
18.8
22.1 (n = 136)
21.4 (n = 28)
21.7 (n = 249)
R–ISS I / II / III,%
16.7/83.3/0 (n = 12)
31.9/59.3/8.8 (n = 113)
18.8/68.8/12.5
31.6/64.0/4.4 (n = 136)
17.9/75.0/7.1 (n = 28)
31.7/61.8/6.4 (n = 249)
Hemoglobin ≤10 g/dL,%
53.8
26.4
31.3
27.6
41.4
27.1
Median ANC x109L (IQR)
3.4 (2.1–4.4)
3.5 (2.7–5.1)
2.6 (1.9–4.1)
3.3 (2.4–4.5)
2.8 (2.1–4.2)
3.3 (2.5–4.7)

Conclusions: Treatment effect was substantially different according to Duffy status and more pronounced than that observed by race. The Duffy antigen has a key role in cytokine/chemokine homeostasis, potentially affecting MM pathobiology and inflammatory stressor responses, thereby providing a biologically plausible rationale for differential treatment effect. Other factors that could contribute to treatment effect differences, e.g. chronic disease prevalence, socioeconomic status, were not formally assessed but eligibility criteria requirements and uniform treatment in DETERMINATION likely minimized these effects. Current analyses are limited by sample size, near–complete concordance of Duffy status with race, and absence of Duffy null White/other race patients, with additional analysis therefore ongoing.
Clinical Trial Registry: ClinicalTrials.gov; NCT01208662
Disclosure: Lauren Merz: none. Rebecca Zon:Triveni Bio-Consultancy, Current equity holder; Primum-Honoraria. Susanna Jacobus:none. Mehmet Samur:none. Jeffrey Zonder:BMS-spouse employment; Regeneron-Consultancy; BMS,Janssen,RLL-Research Funding. Abdullah Khan:BMS, Sanofi-Research Funding, Speakers Bureau; Amgen-Speakers Bureau. Hani Hassoun:none. Larry Anderson: Celgene, GSK, AbbVie, Janssen, Prothena, Sanofi, Beigene, Cellectar, Amgen-Consultancy, Honoraria, Advisory Committees; BMS-Consultancy, Honoraria, Travel Expenses, Research Funding; Celgene, AbbVie, Janssen, Cellectar-Research Funding; Karyopharm-Advisory Committees. Yvonne Efebera: Takeda, Oncopeptides, Alnylam, Sanofi, GlaxoSmithKline, ORCA Therapeutics, BMS/Celgene, Pharmacyclics through Alliance, AFT-Research Funding; Oncopeptides, Sanofi, Janssen Oncology, Pfizer-Consultancy; Takeda, Janssen, Akcea Therapeutics, Alnylum-Speakers Bureau. Tondre Buck:none. Racquel Innis-Shelton: none. Monique Hartley-Brown: BMS/Celgene, Janssen, Sanofi, GSK, AbbVie, MMRF-Consultancy, Honoraria, Research Funding; Cancer Care-Consultancy, Honoraria. Sagar Lonial: AbbVie, Amgen, BMS, Celgene, Genentech, GSK, Janssen, Novartis, Pfizer, Regeneron, Takeda, TG Therapeutics-Advisory Committees; BMS, Janssen, Novartis-Research Funding. Erica Campagnaro:none. Peter Voorhees: Abbvie, GSK, Janssen, Regeneron-Consultancy, Research Funding; AstraZeneca, BMS, Karyopharm, Sanofi, Lava Therapeutics-Consultancy. Robert Orlowski: AbbVie, Adaptive, Asylia Therapeutics, BioTheryX, BMS, DEM BioPharma, Karyopharm, Lytica, Meridian, Monte Rosa, Myeloma 360, Nanjing IASO Biotherapeutics, Neoleukin Therapeutics, Oncopeptides, Pfizer, Regeneron, Sporos Bio, Sanofi, Takeda-Advisory Committees; BMS, CARsgen, Exelixis, Heidelberg, Janssen, Sanofi, Takeda-Clinical Research Funding; Asylia, BioTheryX, Heidelberg-Laboratory Research Funding; Asylia-Patents/Royalties. Edward Libby: Janssen-Research Funding. David Hurd:BMS, J&J, Merck, Pfizer, Proctor & Gamble-equity holder. Caitlin Costello: BMS, Genentech, Janssen, Karyopharm, Kite, Pfizer-Consultancy; BMS, Harpoon, Janssen, Pfizer, Poseida, Takeda-Research Funding; BMS, Janssen, Karyopharm, Kite, Genentech, Pfizer-Honoraria. Noopur Raje: Caribou, Janssen,bluebird, BMS, Celgene, Immuneel, Merck, Novartis, Onyx, Takeda-Advisory Committees; bluebird-Research Funding; Amgen, Laboratories-Steering Committee. Eva Medvedova: none. Philip McCarthy: none. Carter Milner: AstraZeneca, BeiGene, BMS-Speakers Bureau. Cristina Gasparetto: BMS, Karyopharm, Sanofi, Janssen, Amgen, GSK-Advisory Committees; BMS, Karyopharm, Sanofi-Speakers Bureau. Mounzer Agha: none. Krisstina Gowin:none. Rammurti Kamble:none. Sundar Jagannath: Janssen, BMS, Caribou, Legend, Regeneron, Takeda, San ofi, Posieda, GRAIL-Consultancy. Nitya Nathwani: none. Melissa Alsina: BMS, Janssen, Sanofi-Advisory Committees; BMS-Research Funding. Sergio Giralt:none. Jacob Laubach: none. Omar Nadeem: BMS, Janssen, GPCR Therapeutics, Sanofi, Takeda-Advisory Committees; BMS,Janssen, Takeda, J&J-Research Funding; Pfizer-Honoraria. Irene Ghobrial: AbbVie, Adaptive, Aptitude Health, BMS, Novartis, GlaxoSmithKline, Huron Consulting, Janssen, Menarini, Oncopeptides, Pfizer,Sanofi, Sognef, Takeda, Regeneron, Binding Site, CurioScience, Window Therapeutics, 10X Genomics, Amgen, PreDICTA Bioscience-Consultancy; BMS, Janssen, Menarini, Pfizer, Takeda, Regeneron, CurioScience, Vor Biopharma, Amgen-Speaker Fees; PreDICTA Bioscience, Disc Medicine-equity holder, Advisory Committees. Clifton Mo:AbbVie, BMS, GSK, Janssen, Karyopharm, Sanofi, Takeda-Advisory Committees; AbbVie, Janssen, Karyopharm, Sanofi-Consultancy. Kenneth Anderson: Starton Therapeutics,C4 Therapeutics, Dynamic Cell Therapies, Window-Advisory Committees; Janssen, Pfizer, Amgen, AstraZeneca, Genentech-Consultancy. Nikhil Munshi: AbbVie, Adaptive Bio, Amgen, BMS, Celgene, GlaxoSmithKline, Janssen, Karyopharm, Legend Bio, Novartis, Oncopep, Pfizer, Recordati, Sebia, Takeda-Consultancy.
Paul Richardson: Celgene/BMS, GSK, Karyopharm, Oncopeptides, Regeneron, Sanofi-Consultancy; Oncopeptides-Research Funding.
Comments (0)