
Remember me


Background: Haematopoietic stem cell transplantation (HSCT) is a complex, challenging and slow procedure for patients and their families that requires interprofessional collaboration. Therapeutic education programmes play a key role in facilitating the adaptation and management of this process. "Peer-to-Peer education" is an approach based on exchanging of knowledge and experiences between people in similar situations. In addition to the benefits of conventional education, this approach has proven to be especially effective in reducing anxiety and fear, improving understanding and life skills (building confidence and coping mechanisms) among patients with similar and complex treatment. This paper aims to describe the implementation and results of a peer education model in patients who are candidates for HSCT.
Methods: In 2022, Reina Sofia University Hospital in Cordoba (Spain) integrated peer education as part of the existing therapeutic education programme, supported by Escuela Andaluza de Salud Publica. This initiative was structured in two main phases.
Firstly, patients and informal carers who had undergone HSCT were trained as trainers through a workshop guided by expert professionals, based on a previously established educational plan.
Secondly, educational workshops were implemented for patients and informal carers in the pre-HCT phase. These workshops are developed in two sessions of about 180 minutes each and they were carried out in two consecutive weeks. They employed group dynamics such as brainstorming, where trainers noted down key inputs from the participants. Expert nurses and a psycho-oncologist participated as observers, intervening only if inappropriate or erroneous information was expressed. During the sessions, the trained trainers shared their experiences and practical knowledge, creating a peer-learning environment that facilitated strategies for confronting transplantation process.
Results: Preliminary Results
Six workshops were held between March-2022 and October-2024 (table 1):
Table 1: A ttendees at the workshops
Patient
Informal carers
Patient Trainer
Career Trainer
Beneficiaries
WS 1
4
3
2
2
7
WS 2
4
3
2
1
7
WS 3
4
5
2
2
9
WS 4
5
4
2
1
9
WS 5
4
3
2
2
7
WS 6
8
7
2
1
15
A total of 54 people have benefited from the therapeutic education sessions. Additionally, eleven patients and eight carers were trained as trainers.
Conclusions: During this time, many patients and carers have largely benefited of this project. As professionals we have seen that the peer-to-peer education method has proven to be effective in reducing anxiety and improving the coping skills of patients and carers in the pre-PHT phase. Through the exchange of experiences, participants have strengthened their understanding of the process and their emotional well-being.
The training of patients and carers as trainers has ensured the sustainability of the programme, making it a replicable model in other clinical settings for complex procedures such as HSCT.
Further studies are needed to provide the impact of this educational method. In the future, we have undertaken to make a qualitative study of these results.
Disclosure: Nothing to declare
NP002 ADVANCE CARE PLANNING IN CAR-T THERAPY PATIENTS: DEMOGRAPHIC INFLUENCES AND ENGAGEMENT RATES - A RETROSPECTIVE SINGLE-CENTRE STUDY Andres Sebastian Moya Davila 1, Robin Sanderson1, Andrea Kuhnl1, Emil Kumar1, Deborah Yallop1, Jamie Lee1, Orla Stewart1 1King’s College Hospital NHS Foundation Trust, London, United Kingdom of Great Britain and Northern Ireland (the)Background: Advance care planning (ACP) enables patients to discuss their preferences for future medical treatment and care goals with families and healthcare professionals.1 In haematology, chimeric antigen receptor T-cells (CAR-T) have emerged as an effective, sometimes potentially curative treatment for malignancies. However, care focus can rapidly change from curative to palliative, highlighting the importance of early ACP discussions. We aimed to explore whether any measured demographic factors could influence ACP engagement.
Methods: Following local multidisciplinary discussion and National CAR-T Clinical Panel (NCCP) approval, patients proceeded to leukapheresis. During their visit to the apheresis unit, CAR-T clinical nurse specialist introduced ACP principles to all. Patients were then routinely invited to a nurse-led clinic for an ACP discussion before commencing lymphodepletion and subsequent CAR-T infusion.
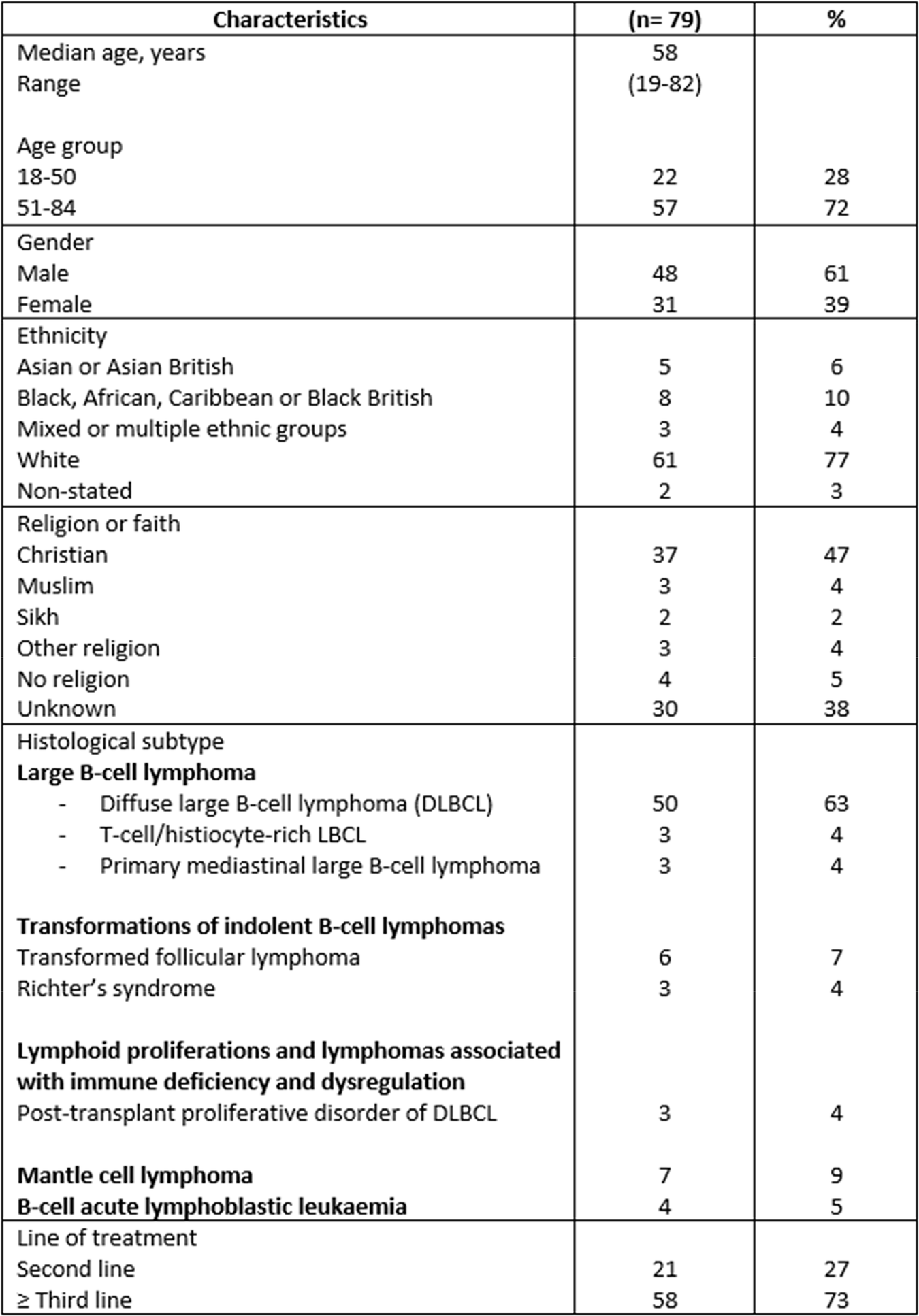
This retrospective single-centre analysis examined data from electronic medical records for 79 consecutive patients who underwent leukapheresis for a commercial CAR-T product between October 2022 and March 2024. Data on ethnicity and religion were classified according to the Office for National Statistics (Census 2021)2,3.
The Chi-square calculator was used to determine the association between categorical variables and analyse the independent relationship between demographic factors and ACP engagement rates.
Results: Sixty-three patients (79.7%) participated in ACP discussions; 44 (69.8%) through video consultations, 8 (12.7%) by telephone and 11 (17.4%) in face-to-face consultations before CAR-T. Most patients (60.3%) preferred having their next of kin or carer present. Engagement rates were comparable between patients receiving CAR-T as second-line therapy (80.9%) and third or later-line therapy (79.3%).
We hypothesised that patients receiving CAR-T in the third or later line would be more amenable to ACP conversations before treatment compared to those in second line. Interestingly, no statistical difference was found between groups (p = 0.87).
Males had a higher participation rate (85.4%) than females (70.9%), though this was not statistically significant (p = 0.11). Similarly, patients aged 51–84 demonstrated greater participation (84.2%) than those aged 18–50 (68.1%) (p = 0.11).

Most ACP participants (71.4%) had a recorded religion or belief; among them, 52.3% stated that faith or belief was irrelevant to them, 41.2% indicated the opposite, and 6.3% had no recorded data. Approximately 80% of patients identified as Christian or had an unknown religion or belief. Among these, 91.8% (34/37) of Christian-affiliated patients participated in ACP compared to 60% (18/30) of those with an unknown religion or belief.
Strong engagement was noted among the two predominant ethnic groups, white (78.7%) and black (75%), collectively accounting for 87% of the study population. Analysis of ACP participation among smaller ethnic and religious groups was limited due to their small representation.
Notably, no ACP participants had an advance care directive, and only 4.7% were known to a hospice or community palliative care pre CAR-T.
Conclusions: Comprehensive conversations around ACP could happen at any stage; however, patients may be better prepared to face all possible outcomes if held before commencing treatment. High engagement across different ethnic and age groups indicates a strong interest towards planning their care in advance of undergoing a potentially life-altering treatment.
Disclosure: Nothing to declare
NP003 ADHERENCE TO IMMUNOSUPPRESSORS AFTER HSCT: A CROSS-SECTIONAL STUDYCaterina Rossi1, Margherita Venturini1, Irene Mansutti1, Marta Vidoni2, Alvisa Palese1, Chiara Visintini 3,2 1University of Udine, Udine, Italy, 2Azienda Sanitaria Universitaria Friuli Centrale, Udine, Italy, 3University of Rome Tor Vergata, Rome, ItalyBackground: Patients receiving an allogeneic hematopoietic stem cell transplant (HSCT) must be adherent to a complex medication regimen including the immunosuppressants, to avoid secondary graft failure and other complications, as the graft-versus-host disease (GvHD). A multidimensional adherence measurement combining subjective and objective measures is recommended. As part of a PhD project, the aim of this study was to assess medication adherence (MA) to oral immunosuppressants using the Basel Assessment of Adherence to immunoSuppressive medIcation Scale© (BAASIS©), a 6-items adherence self‐report instrument and the therapeutic drug monitoring (TDM), as a biochemical indicator of the drug serum concentration. Secondly, the aim was to compare the distribution of adherence data from these two measurement systems.
Methods: A cross-sectional study was conducted. We included adult patients who had undergone an allogeneic HSCT from September 2023 to May 2024 and were in follow-up receiving oral immunosuppressors at the outpatient setting of a Bone Marrow Transplant Centre in the north-east of Italy, discharged from at least one month. Patients were considered adherent if they had answered negatively to all the items of the BAASIS© in the form of interview and if the cyclosporine A (CSA)/tacrolimus (FK) serum concentrations, collected through a central venous catheter or venipuncture, were in the target range (100–250 ng/mL or 5–9 ng/mL, respectively). The Chi-square test was used to compare MA results from the BAASIS© with that from the TDM, with p-value < 0.05.
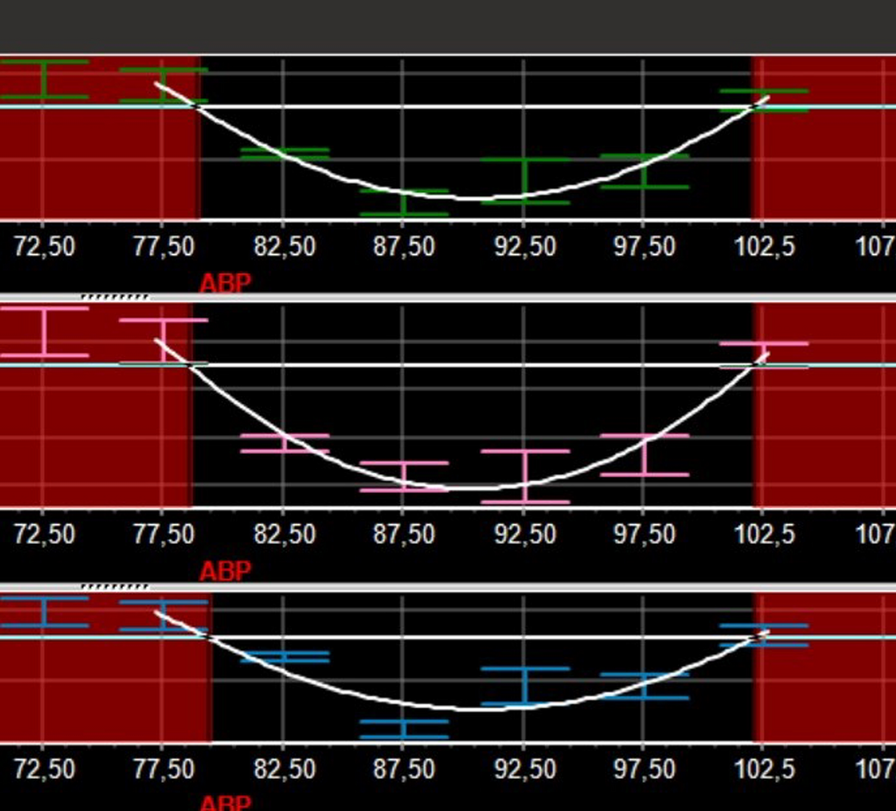
Results: The study included 25 patients, 60% (n = 15) were men with a mean age of 57.8 ± 10.5 years. The most reported indication for HSCT was acute myeloid leukaemia (n = 16, 64%); stem cells came more frequently from a full matched unrelated donor (n = 11, 44%). The mean time from hospital discharge to MA assessment was 51.5 ± 20.5 days and 56% (n = 14) of the patients developed acute GvHD. Almost all the patients were being treated with CSA (n = 24, 96%), only one patient with FK (4%) and 52% (n = 13) of them received also oral prednisone. The proportion of adherent patients was 80% (n = 20) assessed with the BAASIS© and 56% (n = 14) with TDM. Situations of non-adherence observed with the BAASIS© have been shown in Figure 1. No significant difference emerged between MA data from the BAASIS© and from TDM (χ2 = 0.0406, p = 0.84).

Conclusions: Patients undergoing an allogeneic HSCT demonstrated a not very high MA to oral immunosuppressors. These results highlight the need to monitor MA in the clinical practice and to implement strategies to strengthen it. The corroboration between results from the BAASIS© and TDM is not significant, probably due to the small sample size; thus, larger prospective studies, also taking into account the limitation of each MA measurement, are required.
Disclosure: Nothing to declare
NP004 EFFICACY OF A COMPLEX LYSOSTAPHIN GARGLE IN THE PREVENTION OF ORAL MUCOSITIS IN PATIENTS UNDERGOING ALLOGENEIC HEMATOPOIETIC STEM CELL TRANSPLANTATION: A SINGLE-BLIND, RANDOMIZED, CONTROLLED STUDY Xiaoyu Zhou 1, Zhengwen Pan1, Weiwei Zhou1, Weilin Pang1, Liying Zeng1 1The First Affliated Hospital, Zhejiang University School of Medical /Nursing Department, BMT Center, Hangzhou, ChinaBackground: The incidence of OM in patients undergoing myeloablative allogeneic HSCT ranges from 75% to 86.5%.OM not only leads to dry mouth, oral pain, dysphagia, decreased quality of life and increased medical costs, but also may develop into bloodstream infection due to oral infection, which has adverse effects on donor cell implantation and patient prognosis.With the development of nursing technology of HSCT, various physical and chemical sterilization methods have been proved to reduce the incidence of OM. However, in the period of bone marrow suppression of transplantation patients, physical sterilization methods such as brushing teeth often lead to active oral mucosal bleeding in patients with thrombocytopenia and increase the risk of infection; Chemical sterilization methods, such as chlorhexidine mouthwash, have problems such as tooth pigmentation and poor odor, and patients with OM often reduce the compliance of mouthwash due to the painful stimulation of chemical agents on the ulcer surface.Lysostaphin complex is a biological agent, which has been used in burns, diabetic foot and other infectious wounds to verify its efficacy and safety, and the application effect of gargle made of Lysostaphin complex as the main ingredient in HSCT population is unknown.Because of its anti-infective and non-irritating properties, we hypothesized that a complex lysostaphin gargle would be as effective as a chlorhexidine gargle in the prevention of OM in patients undergoing allogeneic HSCT, and would improve patient satisfaction and gargle compliance.
Methods: From January 2020 to December 2021, patients admitted to the bone marrow transplantation center of a third-level first-class hospital in Zhejiang Province, China, for myeloablative allogeneic HSCT were selected by convenience sampling method, and divided into experimental group (n = 200) and control group (n = 200) according to random number table method.The test group was gargled sequentially with 15 ml of sodium bicarbonate gargle and 15 ml of complex lysostaphin gargle, while the control group was gargled sequentially with 15 ml of sodium bicarbonate gargle and 15 ml of chlorhexidine gargle. The incidence of OM, the severity of OM, the time of occurrence of OM, oral pain score, gargle compliance and the time of granulocyte engraftment were compared between the two groups.
Results: Four patients fell out in the experimental group and three patients fell out in the control group, respectively, and 393 patients completed the study.The incidence of OM was 41. 84% in the treatment group and 48. 73% in the control group, with no significant difference between the two groups (P > 0. 05) The incidence of oral pain in the test group was lower than that in the control group (18.8% vs. 28.6%, P < 0. 05), and the incidence of oral pain score ≥ 4 was lower than that of the control group (3.1% vs. 7.6%, P < 0. 05) There was no significant difference in gargle compliance, time of neutrophil implantation and use of analgesic drugs between the two groups.
Conclusions: The staphylococcal enzyme complex gargle has been proved to be safe and effective, and can reduce the incidence and degree of oral pain in patients.
Disclosure: Nothing to declare
NP005 IMPLEMENTATION OF USE OF PERIPHERALLY INSERTED CENTRAL CATHETER (PICC) FOR ADMINISTRATION OF PERIPHERAL BLOOD STEM CELLS (PBSC) IN PATIENTS RECEIVING HEMATOPOIETIC STEM CELL TRANSPLANTATION (HSCT) Yu Ting Ngo 1, Swss Qynn Grace Cham1, Joanne Lee1, Clarice Choong1, Liang Pui Koh1, Lip Kun Tan1, Teck Guan Soh1, Gek Ling Che1, Yoke Lai Tang1, Ana Latip1, Nur Arifah Maziah Binte Moin1, Hui Li Lim1, Jedidiah Lieow1, Eng Soo Yap1, Kwee Cheng Chia1, Michelle Poon1 1National University Cancer Institute Singapore, Singapore, SingaporeBackground: PICC are routinely used for chemotherapy administration, but there is limited data supporting their use for PBSC infusion. Until 2019, despite an existing PICC, our HSCT patients received additional CVC insertion through the internal jugular vein for PBSC infusions. Led by a multidisciplinary team, a stepwise validation/implementation project, through an in-vitro lab based validation process, followed by a clinical review was performed over a 4-year period, evaluating feasibility and safety of using PICC to deliver PBSC to all HSCT patients.
Methods: 1. Lab based validation: In vitro infusion of 6 cryopreserved PBSCs was performed, 3 infused PICC whist 3 via CVC. Each product was thawed for the same amount of time and drained by gravity. Pre-infusion and post-infusion total nucleated cell counts (TNC), CD34 counts and CD34 viability of the PBSCs were analysed by flow-cytometry and compared using paired T test. In vitro infusion rates were also compared between PICC and CVC groups.
2. Clinical outcome analysis: Following the in-vitro lab-based validation process, a first pilot using PICC for PBSC infusion was first performed (between 2019–2020) amongst autologous HSCT (autoHSCT) patients. Data for this was presented previously (Wan et al ASH 2021).
In this final analysis of our project, we extended this initiative to our allogeneic cohort (alloHSCT). Between December 2023 to currently, a 2nd pilot involving 57 alloHSCT patients was conducted. Patient characteristics, time to neutrophil/platelets engraftment, infusion and line-related complications were analyzed.
Results:
1.In vitro findings: Overall flow rates for infusion through PICC was slower (mean 0.1 mls/s vs 0.3 mls/s, p < 0.05). The % differences in TNC counts (5% vs 9%, p = 0.4), CD34 counts (17% vs 15%, p = 0.9) and viability (4% vs 7%, p = 0.2) between pre and post infusion samples for PICC and CVC were however similar.
2.Clinical outcome analysis: Data for the autoHSCT cohort was presented previously (Wan et al ASH 2021), showing comparable engraftement/safety data for the PICC cohort compared to a matched CVC historical cohort. Following this pilot, PICC has been used since 2021, for all autoHSCT with no unexpected safety signals.
For the alloHSCT cohort, 57 patients were included. Table 1 summarized the characteristics of patients included in this study. 26 (45% of patients) had an existing PICC while 31 had PICC inserted for alloHSCT. For patients with existing PICC, median duration of catheter-in-situ was 201 days. No infusion or catheter-related complications were noted in all patients. Median time to neutrophil recovery in the overall, haploidentical cohort and reduced intensity cohort were 14 (range 9–34), 14 (range 9–34) and 11 (range 9–18) days respectively, while median time to platelet recovery were 13 (range 11–28),11 (range 8–28) and 13 (range 10–27) days respectively. These results compared favorably with our historical cohort data.
Table 1: Patient characteristics
Patients N = 57 (%)
Male/Female
35/22
Median Age
52 years old (Range 21–74 years old)
Disease subtype
Acute Leukemia
42 (74)
MDS
7 (12)
Lymphoma
7 (12)
Others
1 (2)
Stem Cell Source
Matched Related Donor
18 (32)
Matched Unrelated Donor
10 (18)
Haploidentical
29 (51)
Conditioning
Myeloablative (MAC)
19 (33)
Reduced intensity (RIC)
38 (67)
Existing PICC*
*median duration of catheter in situ was 201 days
26 (45)
Conclusions: Our findings confirm PICC for PBSC administration in patients receiving alloHSCT is safe, and can reduce additional line insertion in a significant proportion of patients. Our project findings support the implementation of PICC use for PBSC infusion for all HSCT patients, allowing costs reduction and improved safety for our patients.
Disclosure: Nothing to declare
NP006 NURSE LED PRE-HABILITATION FOR PATIENTS UNDERGOING STEM CELL TRANSPLANTATION Jo Preston 1 1Manchester University NHS Foundation Trust, Manchester, United Kingdom of Great Britain and Northern Ireland (the)Background: In 2022 a nurse led pre-habilitation service commenced at Manchester Royal Infirmary (MRI), United Kingdom in conjunction with Anthony Nolan. The service was initiated to ensure patients scheduled for stem cell transplantation (SCT) and families were appropriately prepared, and educated to improve their experience of treatment. Pre-habilitation has shown to benefit patients with solid malignancies (Guerra-Londono CE, 2024), therefore there was enthusiasm to introduce this service to SCT patients, so a new position of pre-habilitation clinical nurse specialist (CNS) was introduced.
Methods: MRI is a tertiary SCT referral center in the Northwest of England serving a population of around 4.9million. MRI treats local patients and those referred from other centers specifically for SCT. Appropriate referral pathways are established and once referred, patients are discussed at regional, virtual and local multi-disciplinary team (MDT) meetings before being accepted for transplant. Once identified as suitable for SCT, the patient is contacted by the pre-habilitation CNS where a telephone consultation is offered. This consultation lasts approximately 1.5 hours and includes all aspects of preparation for transplant. The CNS completes referrals to various MDT members including Physiotherapy, Dietician, Social Worker, Psychological service or other required specialties. The CNS advocates for the patient by coordinating their care prior to SCT, offering advice, support and education through weekly contact until they start conditioning for SCT as an in or outpatient. Patient care is subsequently handed over to the transplant CNS team and the transplant ward, concerns or ongoing issues are identified.
During the weekly contacts with the CNS patients and relatives are counselled on graft versus host disease, fatigue management, post-transplant complications, as well as other patient’s specific requirements. This service is currently offered to those undergoing Allogeneic SCT.
Results: Since 2022 at present (December 2024), 226 patients have been referred to the service, with 16 of those patients not making it to transplant, and 6 patients declining all prehab intervention. This has resulted in 204 patients receiving nurse led prehabilitation before receiving a SCT.
Main themes that come up, are, financial concerns, housing issues, diet and lifestyle issues, and anxiety around treatment.
In 2022 before the implementation of the prehab service average length of stay was 63.7 days, in 2023 the length of stay was 50.1 days. The length of stay for 2024 is in progress.
Patients are sent questionnaires at 3–6 months post SCT depending on their recovery, presently we have received 40 responses. From the questionnaire we can see patients appreciate being prepared for post-transplant complications and felt well supported in the build up to SCT.
Conclusions: The funded prehabilitation CNS role will complete in December 2025. The role has become embedded at MRI and is an important part in preparing the patient for SCT. It has led to patients being better supported, signposted, referred, educated and prepared for SCT. Additional benefits include highlighting financial, psychological and social concerns that could impact patients’ treatment, recovery or discharge.
A business case will be submitted so the role can continue to make a positive impact to patients.
Disclosure: nothing to declare
NP007 PATIENT FEEDBACK ON LYMPHOMA END OF TREATMENT SESSION Katherine Taylor 1 1University College London Hospital (UCLH), London, United Kingdom of Great Britain and Northern Ireland (the)Background: Historically patients who completed treatment for Lymphoma at UCLH had a one hour 1:1 session either in person or via telephone with a Clinical Nurse Specialist (CNS) to discuss their personalised End of Treatment (EOT) Summary. In July 2023 the CNS team started running group EOT sessions. These are small groups of 5–10 patients who have had similar Lymphoma treatments, including patients who have received an Autologous Haematopoietic Stem Cell Transplant (HSCT) sessions are two hours and facilitated by a CNS and MacMillan Support Worker. The session is structured around discussing the EOT summaries as a group and includes videos and a powerpoint containing health promotion advice and signposting to psychological support and resources. Open discussion and questions are encouraged throughout the session and patients are encouraged to participate and share their experiences of diagnosis and treatment if they feel comfortable. The survey was created to evaluate whether patients found a group session useful and if there is any benefit to patients in attending a group session compared with the previous practice of a 1:1 CNS discussion.
Methods: Patients are asked to complete an anonymous feedback survey at the end of the session. This was previously a paper form but is now on Microsoft Forms, patients access it by scanning a QR code on their smart phone. Previously completed paper forms have now been uploaded to MS Forms. Survey contains closed-ended, open- ended and multiple choice questions, there is also space for free text comments.
Results: The feedback survey was created in March 2024, there have been 138 attendees since the feedback form was introduced with 98 responses logged. Of those 138 attendees 25 (18%) had received an Autologous HSCT. The survey asks how patients felt about attending the session with other people who had been treated for Lymphoma 94% answered positively (positive 14% or very positive 80%) 6% answered indifferent or negative. The survey asks if patients felt the session works well in person of if they would have have preferred remote, 80% answered that either remote session would work but they preferred in person (47%) or remote wouldn't work and they preferred in person (33%). 16% of respondents said they would have preferred a remote session, 4% were indifferent. Themes from the free text comments include having a group session earlier in treatment would have helped anxiety, feeling isolated through treatment, hearing other patients experiences was valuable, understanding what symptoms to look out for, lack of psychological support, information on nutrition and lifestyle useful, information on second cancers and healthy lifestyle helpful.
Conclusions: Most patients found attending an in person group EOT session a positive experience. Support for patients at the end of treatment remains an area of unmet need, especially in those who have undergone Autologous HSCT as these patients often face a lengthy period of both physical and psychological recovery. The CNS team intend to continue evaluating and developing the service, and review how support is offered with the aim of improving patients wellbeing after cancer treatment.
Disclosure: Nothing to declare
NP008 CONSTRUCTION OF QUALITY EVALUATION SYSTEM FOR PREVENTION AND NURSING OF DRUG RESISTANT BACTERIAL INFECTION IN HEMATOPOIETIC STEM CELL TRANSPLANTATION PATIENTSQiuhui Zhang1, Jiongtong Fan1, Li Xu1, Ling Zhang1, Na Zhao1, Yuqiu Liu1, Huijuan Zhang1, Guiying Liu1, Wenjun Xie1, Erlie Jiang 1 1Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin, ChinaBackground: Repeated hospitalizations before and after HSCT, long-term neutropenia, and repeated use of broad-spectrum antibiotics all make pathogens susceptible to drug resistance. During HSCT, patients have low immunity and are prone to bloodstream infections. Research has shown that the incidence of bloodstream infections in HSCT patients is 9.2% to 23.3%, which seriously affects the prognosis of patients. Therefore, preventing and controlling the spread of drug-resistant bacteria is the focus of nursing staff in laminar flow wards. Correct assessment is a prerequisite for prevention, and nursing quality assessment, as one of the core contents of nursing management, can improve nursing level while revealing existing nursing problems. Therefore, this study takes Donabedian's "structure process result" three-dimensional quality structure model as the theoretical framework to explore the construction of an evaluation index system for the quality of prevention and care of drug-resistant bacterial infections in HSCT patients, in order to provide reference and inspiration for evaluating the quality of prevention and care of drug-resistant bacterial infections in HSCT patients.
Methods: The domestic and foreign literature, guidelines, and industry standards related to the prevention and nursing of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation were retrieved, and risk factors were extracted;Based on the results of literature retrieval and the work experience of the research team members on the prevention of drug-resistant bacterial infections, a preliminary draft of a nursing quality evaluation system for the prevention of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation was developed. Sixteen multidisciplinary experts were invited to conduct a Delphi expert consultation on the proposed risk indicators, and a final nursing quality evaluation system for the prevention of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation was formed.
Results: The preliminary draft of the quality evaluation system for the prevention and nursing of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation includes 3 primary indicators, 13 secondary indicators, and 70 tertiary indicators.In the two rounds of Delphi expert consultation, the expert activity coefficient was 100% (16/16) and 87.50% (14/16);The expert authority coefficients are 0.888 and 0.910, respectively;Kendall’s W coefficients are 0.196 and 0.205, respectively;In the two rounds of expert consultation, the average importance of each indicator was between 3.688 and 5.000 and between 3.786 and 5.000;The coefficient of variation was 0.000 ~ 0.367 and 0.000 ~ 0.231, and finally a quality evaluation system for nursing care of drug-resistant bacterial infection prevention in hematopoietic stem cell transplantation patients was formed, which included 3 first-level indicators, 12 second-level indicators, and 59 third-level indicators.
Conclusions: The evaluation system for the quality of nursing care for the prevention of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation, which was constructed using the Delphi expert consultation method, is highly authoritative and scientific, and can be used as a basis for comprehensively evaluating the quality of nursing care for the prevention of drug-resistant bacterial infections in patients undergoing hematopoietic stem cell transplantation in clinical practice.
Disclosure: Nothing to declare
NP009 PROPHYLACTIC NASOGASTRIC TUBE FEEDING IN MYELOABLATIVE STEM CELL TRANSPLANT: A SERVICE EVALUATIONVictoria Mace1, Julie Beckerson 1, David Slade1, Lina Johansson2,1 1Imperial Healthcare NHS Trust, London, United Kingdom of Great Britain and Northern Ireland (the), 2Imperial College London, London, United Kingdom of Great Britain and Northern Ireland (the)Background: Myeloablative conditioning (MAC) is toxic to the gastrointestinal tract. MAC causes symptoms such as oral mucositis, nausea, vomiting and diarrhoea which can reduce nutritional intake, causing malnutrition. Due to these side effects, proactive artificial nutrition support (enteral or parenteral nutrition) is required in MAC stem cell transplant (SCT).
Local and international guidelines recommend enteral nutrition over parenteral nutrition due to positive effects on the gastrointestinal mucosa and microbiota. Parenteral nutrition is associated with negative outcomes, such as increased length of stay and risk of infection, prolonged neutrophil engraftment and increased risk of severe gut graft-versus-host disease.
Imperial Healthcare NHS Trust recommends prophylactic nasogastric tube (NGT) insertion for all MAC SCT, prior to the development of oral mucositis. This evaluation describes patient consent, insertion and tolerance of prophylactic NGT and use of parenteral nutrition in MAC SCT patients.
Methods: Retrospective single-centre analysis on all patients following MAC SCT at Hammersmith Hospital between November 2022 and November 2024. Data were collected from digital patient records on demographics, conditioning regimen, donor type, date of insertion and complications of NGT, pre-SCT workup clinic discussion about NGT, consent for NGT, and use of parenteral nutrition.
Results: All patients (n = 31) who underwent a MAC SCT Hammersmith Hospital between November 2022 and November 2024 were analysed. Median age was 41 years (range 22–53). Sixteen (52%) were sibling or matched unrelated donors and 15 (48%) were haploidentical.
Consent for NGT insertion was given by 23 patients. Of these, 6 (23%) did not tolerate the insertion, 2 (9%) could not tolerate the NG feed due to nausea/feeling full, 6 (23%) vomited out the NGT after 1–8 days. One (4%) patient consented to a NGT reinsertion (after vomiting it out). Ten (31%) patients met nutritional requirements with enteral nutrition. Detail on those that had parenteral nutrition and oral intake only and further results are detailed in Table 1.
Table 1: Summary of consent for NGT and route of ANS for myeloablative allogeneic stem cell transplant.
Demographics
Consent to NGT
Did not consent to NGT
All, n = 31 (%)
23 (74)
8 (26)
Female n = 8 (%)
8 (100)
0
Male n = 23 (%)
15 (65)
8 (35)
NGT was discussed in pre-SCT workup clinic
Yes. n = 18 (%)
13 (72)
5 (28)
No n = 13 (%)
10 (77)
3 (23)
Route of ANS
No ANS (oral intake only)
Enteral nutrition
Enteral and parenteral nutrition
Parenteral nutrition
n = 31 (%)
5 (16)
10 (32)
2 (6)
14 (45)
Reason for starting parenteral nutrition
Did not consent NGT
Did not tolerate NGT insertion
GI intolerance of enteral nutrition (vomited NGT/feeling full)
Mucositis prevented NGT insertion
Parenteral nutrition n = 16 (%)
6 (38)
3 (18)
6 (38)
1 (6)
NGT = naso-gastric tube, SCT = stem cell transplant, GI = Gastrointestinal, ANS = Artificial nutrition supportConclusions: Enteral is the recommended route of artificial nutrition support in SCT patients, however only one third (32%) of this cohort met their nutritional requirements this way. Over half (51%) required parenteral nutrition. 40% of patients who had parenteral nutrition did not consent for NGT. Understanding the reasons patients refused NGT insertion may identify areas for improvement in the consenting process. Other reasons for parenteral nutrition were gastro-intestinal side effects such as nausea, vomiting or not tolerating insertion of the NGT. Enteral nutrition may be better tolerated if there was improved pharmacological and multi-disciplinary management of these symptoms.
There is scope to significantly improve the acceptance and tolerance of the prophylactic NGT. Future improvement projects could include exploring the consenting process, medical management of symptoms and alternative routes of enteral nutrition such as naso-jejunal feeding. This may decrease use of parenteral nutrition in this cohort, and associated complications such as prolonged admissions, infection and gut graft-versus-host disease.
Clinical Trial Registry: Audit no: ASM HH_31
Disclosure: Nothing to declare
NP010 'BACK TO SCHOOL': CAN A STEM CELL TRANSPLANT EDUCATION PROGRAM ENHANCE PATIENT EXPERIENCES? Christina Paula Tejada 1 1University College London Hospital, London, United Kingdom of Great Britain and Northern Ireland (the)Background: Stem cell transplants have been used for decades as potentially curative treatment for some malignant and benign conditions. This complex process replaces damaged cells by infusing healthy stem cells from a donor (allogeneic) or oneself (autologous stem cell transplant (ASCT)) (Balassa et al. 2018). In the last 3 years, University College Hospital has accepted over 300 ASCT referrals. Lymphoma patients referred for ASCT often lack sufficient knowledge about ASCT. Due to time constraints and limited unit capacity, they typically receive most of the necessary information during their first appointment. Such an approach can negatively impact patient experiences and pose a barrier to obtaining informed consent (IC). To facilitate IC, which aligns with patient centred care and encourages autonomy (Griffith, 2024), nurses must provide information that is easy to understand, educates on risks and alternatives, supports communication needs, upheld by current evidence, and allows ample discussion time (Care Quality Commission, 2023).
Methods: Acknowledging this deficit, between May and November 2024, an interactive education session named ‘Auto School’ was created by lymphoma nurse specialists for lymphoma patients. Patients were encouraged to attend with their next of kin for support. This session comprised of a PowerPoint and information packs discussing topics on:
Two locally designed questionnaires were provided to patients: one after the education session, and another to those who also completed ASCT.
Results: 17 patients attended ‘Auto School’ following which 6 patients have already undergone ASCT and 7 patients still waiting to proceed. 3 patients did not proceed due to disease progression. 1 patient felt that the education session facilitated an informed decision to decline ASCT. From the 17 post session questionnaires completed, patients were very satisfied with the pace and content of information and understood all topics discussed within the given time. There was no feedback on session improvement.
For the 6 ASCT patients, only 3 post-transplant questionnaires were completed providing a limited view of data. However, the data highlighted common themes that the education session helped to prepare patients for their ASCT, promoted patient-centred care and empowered autonomous decision making. Patients felt challenging discussions related to infections, intensive care admission and death were discussed appropriately, helping to manage expectations about potential outcomes. However, felt certain topics such as recovery, being discharged home and psychosocial support for families were not explored in depth.
Conclusions: Patients appreciate the opportunity to be counselled on sensitive topics prior to consenting (Hockings and Peggs, 2013). However, with ASCT, a great deal of emphasis is often placed on the procedure with insufficient education on psychosocial effects, which have the capacity to reduce morbidity and recovery time (Hamandi et al., 2010). Overall, ‘Auto school’ achieved its objectives of improving patient experiences as well as managing patient expectations and facilitating IC. Therefore, structured education, exploring procedure and available psychosocial support may have potential to further improve patient’s experiences with ASCT.
Disclosure: Nothing to declare
NP011 HAEMATOLOGY EMERGENCY DEPARTMENT UTILIZATION AFTER ALLOGENEIC HEMATOPOIETIC STEM CELL TRANSPLANTATION: A SINGLE-CENTER EXPERIENCE Cristina Canaleta 1, Alba Pla1, Albert Esquirol1, Irene Garcia-Cadenas1, Elisabeth Lazaro1, Eva Iranzo1, Olga Aso1, Mercè Triquell1, Javier Briones1, Núria Font1 1Hospital de Sant Pau, Barcelona, SpainBackground: The haematology emergency department (HED) plays a key role in managing patients with haematological diseases, particularly allogeneic stem cell transplant recipients (allo-HSCT), whose clinical complexity demands specialized care. At our center, a dedicated Day Hospital provides specialised care for high-complexity patients, reducing reliance on general emergency services. This model aims to minimize waiting times reduce nosocomial infection risks and improve quality of life during the therapeutic process. Patient triage is conducted by nursing staff, who assess clinical needs and coordinate care with the medical team.
Methods: Objective: To analyze the frequency and main reasons for emergency consultations among allo-HSCT patients in the HED of Hospital de la Santa Creu i Sant Pau (HSCSP) from January 2023 to October 2024.
Observational, descriptive study within the HDE of a tertiary hospital performing around 50 procedures per year. Data were extracted from patients records during the study period, analysing variables such as: consultation reasons, triage priority, and subsequent management. Patients were classified into two groups: early post-HSCT (<1 year) late post-HSCT (>1year).
Results: A total of 1786 episodes were cared for at the HED during the study period, of which 477 episodes (26.71%) were allo-HSCT recipients and 188 (39.41%) were in the early post-HSCT group.
The most frequent consultation reasons were respiratory symptoms (n = 130, 25.9%), fever (n = 97, 19.3%), skin manifestations (n = 70, 13.9%) and pain (n = 49, 9.8%). Early post-HSCT episodes included more frequently febrile episodes (23.2% vs 16,8%, p = 0.103) and skin manifestations suggestive of GVHD (19.6% vs 10,39%, p = 0.006). Late post-HSCT episodes primarily presented with respiratory symptoms (n = 106, 34.4%) and fever (n = 52, 16.8%).
Overall, 136 cases (28.5%) were classified as high priority requiring additional tests. Hospital admission was required in 59 (43.4%), while 56.62% were managed on an outpatient basis. Among early post-HSCT episodes, 43.6% were high priority cases, with 34.1% requiring hospital admission. For late post-HSCT patients, 18.7% were high priority, with 53.7% requiring admission.
Reason for consultation
Early post-HSCT
Late post-HSCT
p-value
N = 194
N = 289
Diarrhoea
22 (11,3%)
22 (7,1%)
0.145
Nausea/Vomiting
4 (2,1%)
5 (1,6%)
0.739
Fever
45 (23,2%)
52 (16,9%)
0.103
Skin-related event
38 (19,6%)
32 (10,4%)
0.006
Respiratory symptoms
24 (12,4%)
106 (34,4%)
<0.001
Pain
12 (6,2%)
37 (12%)
0.047
Anaemia/Fatigue
10 (5,2%)
18 (5,9%)
0.898
Others (cystitis, oedema, epistaxis, voiding syndrome, mucositis...),
39 (20,1)
36 (11,7%)
0.014
Conclusions: This study highlights the high volume of HED consultations among allo-HSCT patients, reflecting their clinical complexity, Early post-transplant episodes were more likely to be high-priority cases, particularly involving fever and skin lesions, requiring close monitoring and specialized care. In contrast, late post-transplant episodes often required admission for respiratory symptoms. These findings underscore the crucial role of nursing-led triage and tailored care approaches in improving patient outcomes and optimizing healthcare resource utilization in haematology emergency care.
Disclosure: Nothing to declare
NP012 UTILIZING DIGITAL THERAPEUTIC EDUCATION FOR ADOLESCENTS AND YOUNG ADULTS UNDERGOING HEMATOPOIETIC STEM CELL TRANSPLANTATION: A SCOPING REVIEW OF EVIDENCE AND STRATEGIES Simona Calza 1, Carlotta Neri1, Marco Deiana1, Evelina Olcese1, Giulia Ottonello1, Silvia Rossi1, Roberta Da Rin Della Mora1, Nicoletta Dasso1, Raffaella Garbarino1, Giulia Pessina1, Ilaria Artuso1, Giuseppe Minniti Caracciolo1, Silvia Scelsi1 1IRCCS Istituto Giannina Gaslini, Genoa, ItalyBackground: Therapeutic education is essential in supporting adolescents and young adults (AYA) with hematologic-oncologic conditions, including those undergoing transplantation. This approach enhances disease understanding, treatment adherence, and quality of life while addressing the complex clinical and psychosocial needs of this population. Healthcare professionals play a pivotal role in implementing tailored educational interventions, which are increasingly augmented by innovative digital tools such as QR codes and online platforms. This scoping review aims to map the available evidence on the role of nurses in therapeutic education for AYA with hematologic-oncologic conditions, focusing on the impact of digital tools and the optimization of interventions for transplanted patients.
Methods: The scoping review was conducted using Arksey and O’Malley ‘s framework. The PRISMA 2020 guidelines were also applied to ensure transparency and rigor throughout the process. Searches were performed in PubMed, CINAHL, Web of Science, and Scopus using keywords such as "therapeutic education," "AYA," "hematologic-oncology," "transplantation," and "healthcare professional."
Results: A total of n = 418 articles were initially identified, with n = 53 meeting relevance criteria. Of these, n = 6 studies were included in the final analysis. The results highlight the significant impact of therapeutic education on improving autonomy, treatment adherence, and disease management among AYA.
Digital tools, such as QR codes and online platforms, were found to provide structured and personalized educational pathways, enhancing information accessibility and continuity of care. For transplanted patients, these tools proved particularly effective in managing post-transplant complications, optimizing clinical outcomes, and mitigating associated risks. Healthcare professionals play a critical role in tailoring these interventions to meet individual patient needs and in facilitating effective communication with patients and their families.
Conclusions: This scoping review confirms the value of digital approaches in therapeutic education for AYA with hematologic-oncologic conditions, including transplanted patients. Digital tools enhance the effectiveness of educational interventions, empowering patients in self-management and ensuring continuity of care.
To integrate these strategies effectively into clinical practice, significant investments are required in training healthcare professionals and developing adequate technological infrastructures. Evidence-based educational approaches, such as those identified in this review, strengthen the position of healthcare professionals as key facilitators of patient-centered care, contributing to improved clinical outcomes and enhanced quality of life for patients.
Reference: Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
Disclosure: none
NP013 NURSE LED CLINIC HEMATOLOGY: DREAMWORK OR TEAMWORK Maaike De Ruijter 1, Annemarie Overbeek2, Vanessa ter Haar3 1AmsterdamUMC Vumc, Amsterdam, Netherlands (the), 2Spaarne Gasthuis, Hoofddorp, Netherlands (the), 3OLVG, Amsterdam, Netherlands (the)Background: A nurse-led clinic hematology is a healthcare model where advanced practice nurses, specialized in hematology, lead the clinical management of patients, primarily focusing on those with chronic diseases. These clinics emphasize patient assessment, treatment management, education, and long-term care. Nurses in these clinics conduct physical examinations, monitor lab results, administer treatments, and provide patient education on managing their conditions. The model highlights a multidisciplinary approach, collaborating with physicians and other healthcare professionals to optimize care. Nurse-led clinics improve access to care, enhance patient satisfaction through personalized attention, and offer cost-effective management of chronic diseases.
The treatment process surrounding autologous stem cell transplantation primarily involves standardized care, making it ideally suited for a nurse-led clinic. Patients requiring autologous stem cell transplantation were previously treated by hematology residents or fellows, meaning different doctors were involved throughout the process due to changing shifts and responsibilities.
The nurse-led clinic not only improves patient outcomes but also ensures continuity of care, reducing complications and hospital admissions.
Methods: When patients are diagnosed with a hematological disease and high-dose chemotherapy followed by autologous stem cell transplantation (ASCT) is indicated, they are referred to a transplant center. In the Amsterdam region, patients are referred to Amsterdam UMC, location VUmc. From that point onward, a nurse practitioner leads the treatment process under the supervision of a hematologist.
Key moments of care and contact occur at various stages, including before apheresis, during apheresis, before the autologous transplant, and during high-dose chemotherapy and stem cell reinfusion, which can take place either in the clinic or the outpatient clinic at VUmc. After the transplant, follow-up care is p
Comments (0)