Study Design
The study designs, including full inclusion/exclusion criteria, treatment protocols, safety outcomes and adverse events, for the COAST-V (NCT02696785), COAST-W (NCT02696798), and COAST-X (NCT02757352) studies have been previously published [12,13,14]. Briefly, COAST-V, COAST-W, and COAST-X were phase 3, multicenter, randomized, double-blind, and placebo-controlled trials evaluating the efficacy and safety of ixekizumab in patients with r-axSpA (COAST-V and COAST-W) or nr-axSpA (COAST-X). COAST-V and COAST-W were double-blinded from baseline to week 16; COAST-X was double-blinded from baseline to week 52.
Patients were randomly allocated to receive 80 mg ixekizumab every 2 weeks (Q2W), 80 mg ixekizumab every 4 weeks (Q4W), or placebo via subcutaneous administration. Patients randomized to the ixekizumab treatment regimens were randomized (1:1) to receive either an 80‐mg or 160‐mg starting dose of ixekizumab at week 0. In COAST-V, there was an additional active-reference arm in which patients were treated with 40-mg adalimumab Q2W. At week 16 in the COAST-V and COAST-W studies, patients who initially received adalimumab (COAST-V only) or placebo were re-randomized 1:1 in a double-blinded manner to receive ixekizumab Q2W or ixekizumab Q4W through week 52. In COAST-X, patients could switch to open-label ixekizumab Q2W after week 16 at the discretion of the principal investigator.
Ethical Approval
COAST-V, COAST-W, and COAST-X (ClinicalTrials.gov identifiers: NCT02696785, NCT02696798, and NCT02757352, respectively) were approved by the institutional review board or ethics committee at each site and were conducted in accordance with the ethical principles of the Declaration of Helsinki and Good Clinical Practice Guidelines (CPMP/ICH/135/95). The master ethics committee was Schulman Associates IRB, (Cincinnati, OH, USA). Full listings of investigators and sites are available in previously published manuscript supplements [14, 15, 17]. All patients gave written informed consent before the trials started. No additional ethical approval was sought to conduct the current post hoc analysis.
Patients
Patient eligibility criteria have been described in previous publications [12, 13, 15]. Briefly, eligible patients were ≥ 18 years of age with a diagnosis of axSpA. In COAST-V (N = 341) and COAST-W (N = 316), patients were required to meet ASAS criteria for r-axSpA (with a centrally read radiograph showing sacroiliitis using the modified New York criteria and at least one spondyloarthritis feature; the central reading was conducted by two readers and an adjudicator in case of a discrepancy). In COAST-W, patients were required to have a treatment history for axSpA of at least 12 weeks. In COAST-X (N = 303), patients were required to meet ASAS criteria for nr-axSpA and have a treatment history for axSpA of at least 12 weeks; all magnetic resonance imaging (MRI) scans and radiographs for COAST-X were centrally read. Patients with radiographic sacroiliitis meeting the modified New York criteria were excluded from COAST-X.
Patients in COAST-V and COAST-X were required to be bDMARD (biologic disease-modifying antirheumatic drug)-naïve. In COAST-W, patients were required to have discontinued one or two TNFi therapies because of intolerance or inadequate response.
Assessments
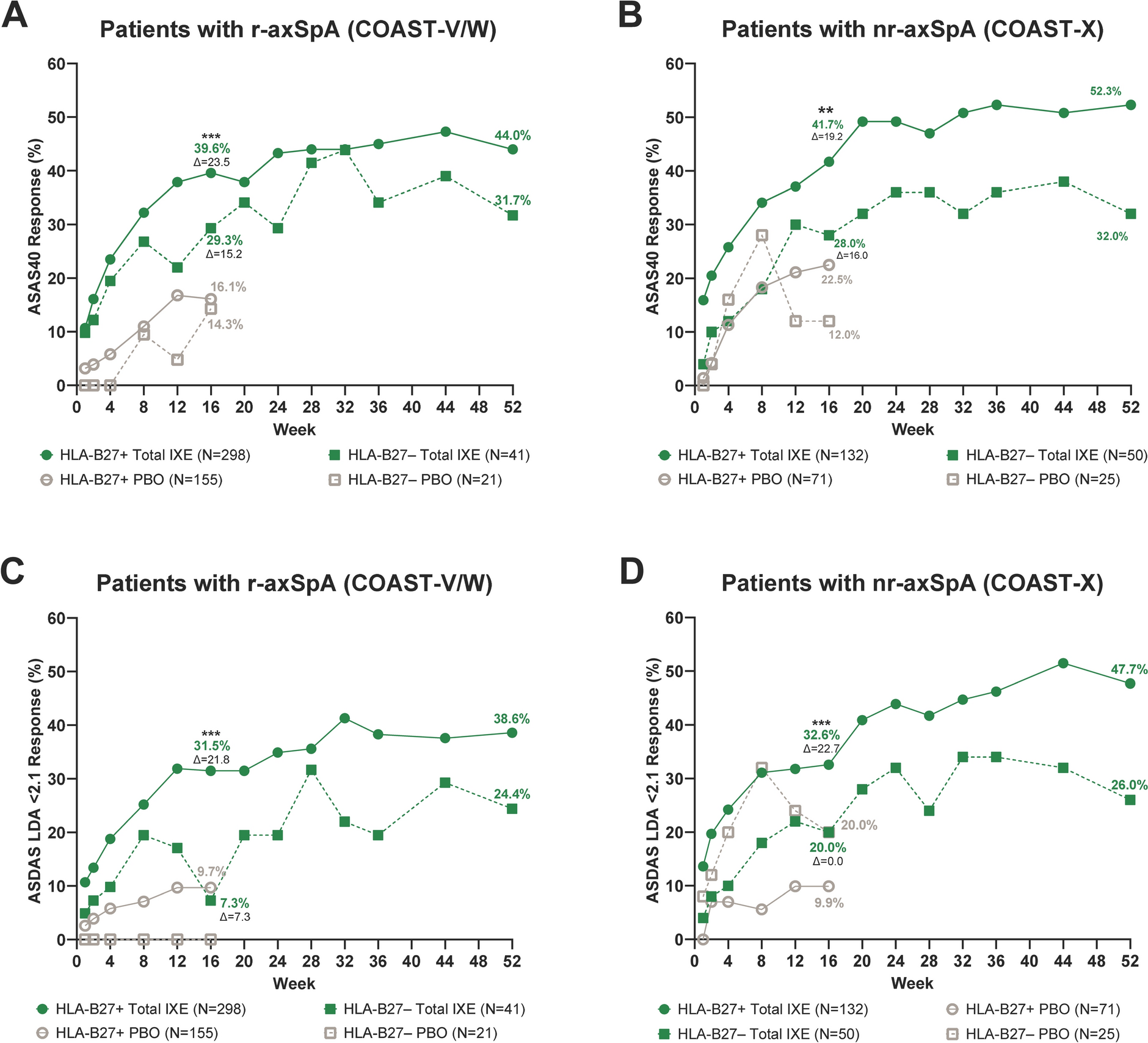
In this post hoc analysis of patients in COAST-V and COAST-W (r-axSpA) and COAST-X (nr-axSpA), we assessed the efficacy of ixekizumab in patient subgroups based on HLA-B27 carrier status (positive/negative) through week 16 and descriptively summarized efficacy response by HLA-B27 status subgroups through week 52.
Efficacy was measured by the proportion of patients who achieved ≥ 40% ASAS improvement (ASAS40), the proportion of patients with an Axial Spondyloarthritis Disease Activity Score (ASDAS) of low disease activity (LDA [defined as < 2.1]), mean change from baseline in the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and the proportion of patients with ≥ 50% improvement from baseline in the BASDAI score (BASDAI50). We also assessed the mean change from baseline in the Short Form-36 Health Survey Physical Component Summary (SF-36 PCS) score.
Statistical Analysis
Patients in the intent-to-treat population who met protocol eligibility criteria were included in this analysis (i.e., patients with protocol deviations related to inclusion and exclusion criteria were excluded). Data from COAST-V and COAST-W were integrated, and COAST-X data were analyzed separately. In COAST-X, patients who received ixekizumab or placebo could switch to open-label ixekizumab Q2W after week 16 at the discretion of the principal investigator [13]. Patients initially randomized to ixekizumab who switched to open-label treatment were included in analyses for the total ixekizumab group (combined Q4W and Q2W treatment arms).
Baseline demographics, disease characteristics, and MRI results of the spine were described by HLA-B27 status for the placebo and total ixekizumab groups.
We evaluated the proportion of patients who achieved ASAS40, ASDAS LDA, BASDAI50, and the mean change from baseline in BASDAI and SF-36 PCS through week 16, including statistical comparisons versus placebo, and summarized the data through week 52.
For the integrated COAST-V and COAST-W analyses, the treatment comparison between the ixekizumab treatment arms and placebo at week 16 within each HLA-B27 subgroup was performed using the Cochran–Mantel–Haenszel test for categorical variables, stratified by study, and an analysis of covariance model for continuous variables with baseline value, study, and treatment as variables. For the COAST-X analyses, the treatment comparison between the ixekizumab treatment arms and placebo at week 16 within each HLA-B27 subgroup was performed using Fisher’s exact test for categorical variables and the analysis of covariance model for continuous variables with baseline value and treatment as variables. Missing data were imputed using non-responder imputation and modified baseline observation carried forward for categorical and continuous variables, respectively. The magnitude of benefit was calculated as the response rate or change from baseline for ixekizumab-treated patients minus that for placebo-treated patients at week 16. Analyses were conducted with SAS® version 9.2 or higher (SAS Institute, Cary, NC, USA).



Comments (0)