
Remember me
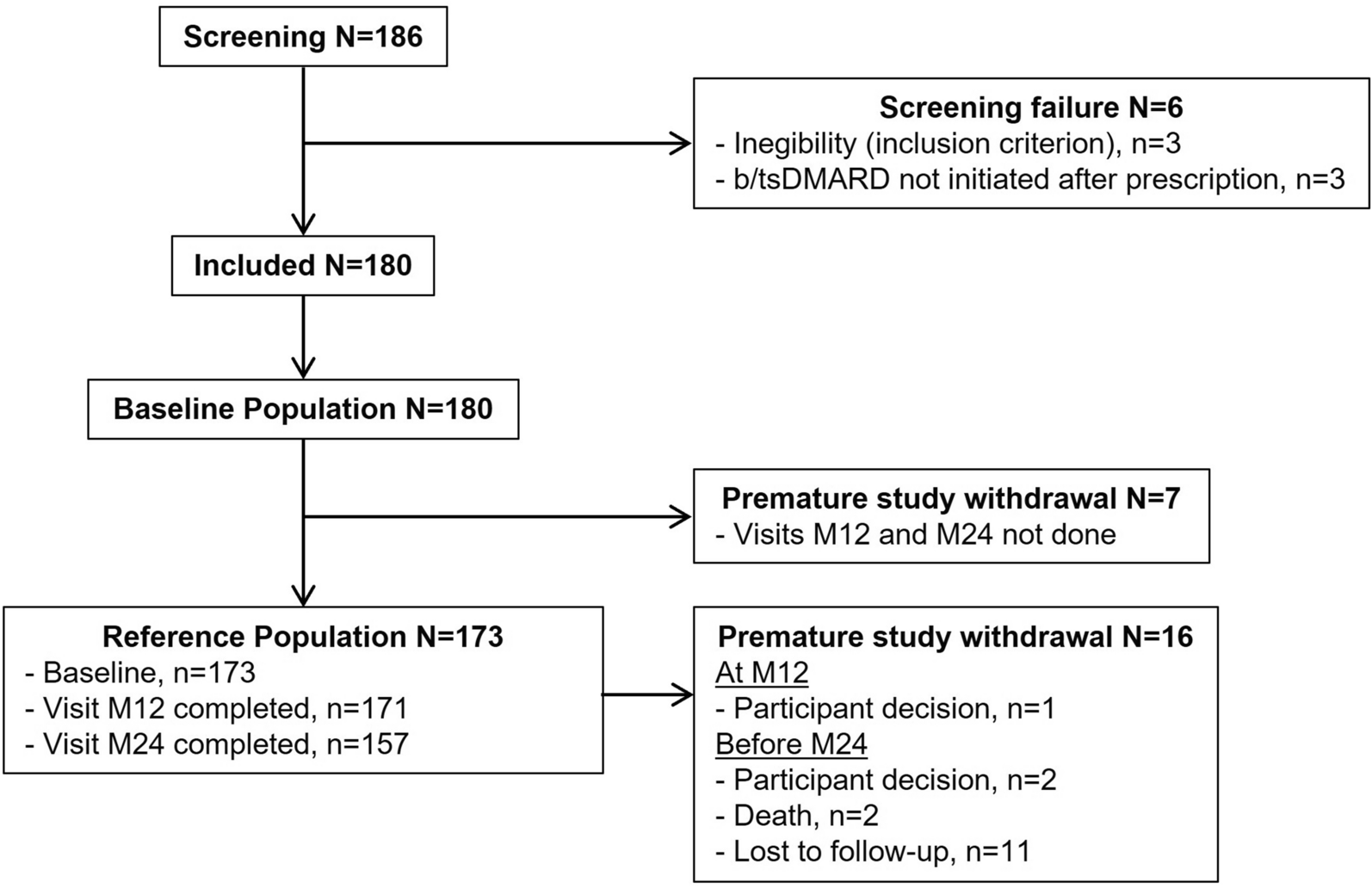


Of the 186 participants screened, 3 were deemed ineligible on the basis of the inclusion criteria, and 3 did not initiate b/tsDMARD therapy despite receiving a prescription at inclusion (Fig. 1). The study enrolled 180 eligible participants; however, 7 participants withdrew prematurely without completing the M12 or M24 follow-up visits. Thus, baseline characteristics were reported, and outcome analyses were conducted on a reference population of 173 participants. Of these, 171 (98.8%) participants completed the M12 visit, and 157 (90.8%) completed the M24 visit. One (0.6%) participant withdrew during the M12 visit, while 15 (8.7%) withdrew before the M24 visit. Among those who withdrew prior to M24, 11 participants were lost to follow-up, 2 participants decided to withdraw, and 2 participants died.
Fig. 1
At baseline, the reference population (N = 173) consisted of 130 (75.1%) women and 43 (24.9%) men, with a mean (SD) age of 56.1 (13.7) years (Table 1) and a mean (SD) time since RA diagnosis of 5.6 (7.3) years. The overall mean (SD) DAS28 score was 4.3 (1.2), with 32 (19.0%) participants classified as having low disease activity and 14 (8.3%) participants in remission.
Table 1 Demographics and baseline characteristics of the study participantsOverall, first-line treatment for RA was initiated, on average, 4.3 (SD 5.4) years prior to study inclusion. MTX was prescribed as the first-line treatment for 150 (86.7%) participants (Table 2). Approximately two-thirds (n = 114, 65.8%) of participants had started MTX more than 1 year before inclusion. At baseline, the mean (SD) weekly dose of MTX was 18.8 (4.2) mg (median 20.0), primarily administered subcutaneously (n = 125, 72.3%), while 47 (27.2%) participants took it orally, and only 1 (0.6%) participant received it via intramuscular injection.
Table 2 RA treatments at baselineTreatments associated with MTX included corticosteroids (CS) for 86 (50.0%) participants, with a mean daily dose of 9.6 mg (median 7.5).
Primary OutcomeMaintenance of MTX Treatment 1 Year After b/tsDMARD InitiationAt the M12 follow-up visit, the same treatment modalities for MTX were maintained in 69 participants, corresponding to 39.9% (95% CI 32.5–47.6) of the study population (Table 3). In contrast, MTX treatment was modified or discontinued for 104 (60.1%, 95% CI 52.4–67.5) participants.
Table 3 Maintenance, modification, or discontinuation of MTX treatment after b/tsDMARD initiationSecondary OutcomesMaintenance, Modifications, or Discontinuation of MTX TreatmentOne year after b/tsDMARD initiation, 144 (83.2%) participants were still treated with MTX (Table 3). Specifically, 69 (39.9%) participants maintained the same dosage and route of administration, while 75 (43.3%) participants experienced changes in their MTX treatment modalities—either in dosage, route of administration, or both. MTX was discontinued in 29 (16.8%) participants at the M12 visit. Modification strategies for MTX treatment, listed in order of prevalence, included a dosage reduction alone (n = 45, 26.0%), a combination of dosage reduction and change from subcutaneous to oral administration (n = 25, 14.4%), and a change from subcutaneous to oral administration alone (n = 5, 2.9%).
Two years after b/tsDMARD initiation, 118 (75.2%) participants remained on MTX (Table 3). A total of 54 (34.4%, 95% CI 27.0–42.4) participants maintained the same dosage and route of administration, while 103 (65.6%, 95% CI 57.6–73.0) participants had either modified their treatment or discontinued MTX by the M24 visit. Specifically, 64 (40.7%) participants received a modified MTX treatment, and 39 (24.8%) discontinued MTX entirely.
Modification strategies at M24 were similar to those employed at M12, including dosage adjustments and changes to the route of administration.
Therapeutic Decisions After b/tsDMARD InitiationAt inclusion, rheumatologists prescribed the following types of b/tsDMARDs: 100 (57.8%) anti-tumour necrosis factor (anti-TNF), 30 (17.3%) Cytotoxic T-lymphocyte antigen 4 - immunoglobulin (CTLA4-Ig), 18 (10.4%) tsDMARDs (JAKi), and 3 (1.7%) anti-B-cell (anti-CD20) (Table 4). Concomitantly, MTX treatment was maintained for most participants (n = 169, 97.7%), either with unchanged modalities or with modifications to dosage or route of administration. The mean (SD) weekly MTX dosage was 17.8 (4.5) mg, with 112 (66.3%) participants receiving it via subcutaneous injections and 56 (33.1%) via oral administration. Nearly half of the participants (n = 81, 47.1%) continued CS treatment at the time of b/tsDMARD initiation.
Table 4 Therapeutic decisions since b/tsDMARD initiationThe continuation of b/tsDMARD therapy was observed in 159 (91.9%) participants at the M12 visit and 132 (84.1%) participants at the M24 visit (Table 4). Of the 132 participants followed at M24, 86 (65.2%) remained on the same b/tsDMARD therapy, while 32 (24.0%) received a second-line treatment, 11 (8.3%) a third-line treatment, and 3 (2.3%) a fourth-line treatment. Anti-TNF therapy remained the most frequently prescribed b/tsDMARD. However, its use tended to decrease compared to baseline, with 74 (46.5%) prescriptions at M12 and 54 (40.9%) at M24. Treatment cessations were primarily reported for anti-TNF therapies. At M12, 31 (19.5%) participants were still treated with other bDMARDs, and this proportion remained stable at M24 (n = 28, 21.2%). Anti-IL-6 therapies represented 27 (17.0%) treatments at M12 and 25 (18.9%) treatments at M24. Furthermore, tsDMARDs comprised 27 (17.0%) treatments at M12 and 23 (17.4%) treatments at M24.
Adaptations to MTX treatment included both dose reductions and changes in the route of administration (Table 4). By M12, the mean (SD) weekly MTX dosage had decreased to 15.9 (4.5) mg. Subcutaneous injections became less common (n = 79, 54.9%), while oral administration increased (n = 63, 43.8%). Similarly, at M24, the mean (SD) weekly MTX dose was 15.8 (4.6) mg, administered subcutaneously to 66 (55.9%) participants and orally to 50 (42.4%) participants.
Rheumatologists suspended CS therapy in 91 (52.9%) participants at the initiation of b/tsDMARD (Table 4). This proportion increased to 105 (61.0%) participants at M12 and 97 (62.2%) participants at M24. Nevertheless, among those who continued CS therapy, the mean (SD) daily dose remained relatively high throughout the study: 9.3 (7.5) mg at b/tsDMARD initiation, 8.9 (9.0) mg at M12, and 9.3 (9.3) mg at M24.
Reasons Driving MTX DiscontinuationMTX discontinuation was reported in 29 (16.8%) participants during the first year and 39 (24.8%) participants during the second year following b/tsDMARD initiation. At both time points, the primary reasons for discontinuation were participant decisions (M12: n = 11, 39.2%; M24: n = 14, 35.9%) and adverse events (M12: n = 10, 35.7%; M24: n = 13, 33.3%) (Supplementary Table S1). No unexpected safety concerns or serious adverse events related to MTX or b/tsDMARDs were reported during the study (Supplementary Table S2).
Factors Favouring the Maintenance of MTX TreatmentThe factors associated with the decision to maintain MTX treatment with the same modalities, from the initiation of b/tsDMARDs to the M24 follow-up visit, were investigated using univariate logistic regression analysis (Supplementary Table S3). Factors with a p > 0.200 were excluded from further analysis to focus on significant predictors. Among the factors assessed, receiving a prescription at baseline for combination therapy versus b/tsDMARD monotherapy (reference) was not significantly associated with MTX maintenance during the first 2 years of b/tsDMARD therapy (OR (95% CI) 1.02 (0.53–1.98), p = 0.952).
Multivariable analysis identified two significant predictors for MTX maintenance at M24. Participant age was identified as a factor, with each additional year of age significantly increasing the likelihood of maintaining MTX (OR (95% CI) 1.04 (1.01–1.08), p = 0.011, Supplementary Table S4). Furthermore, each additional unit on the visual analogue scale measuring participant-perceived disease activity was significantly associated with an increased likelihood of maintaining MTX (OR (95% CI) 1.02 (1.00–1.04), p = 0.005).
Non-smoking was not significantly associated with MTX maintenance (OR (95% CI) 1.95 (0.66–5.78), p = 0.231), although it was included as a potential predictor in the analysis. Therapeutic decisions made by rheumatologists practising exclusively in hospital-based settings, as opposed to those in private practice with partial hospital involvement (reference), were also not significantly associated with MTX maintenance (OR (95% CI) 2.94 (0.98–8.85), p = 0.055). Finally, given the multicentric design of this study, the centre effect was tested and found to be non-significant, indicating that rheumatologist practices were consistent across geographic locations.
Evolution of Disease Activity and Participants’ Physical Function Since b/tsDMARD InitiationSince b/tsDMARD initiation, the DAS28 score progressively decreased over time, with mean (SD) changes from baseline of − 1.7 (1.4) at M12 and − 2.0 (1.3) at M24 (Table 5). The number of participants in remission increased from 14 (8.3%) at baseline to 81 (53.3%) at M12, and further to 95 (66.0%) at M24. In contrast, 49 (34.7%) participants did not achieve low disease activity by M24, with 27 (19.1%) displaying a moderate response and 22 (15.6%) showing no response to therapy. Reduction in disease activity (DAS28) and improvement in physical function (HAQ-DI) were observed within similar ranges across groups, regardless of whether MTX was maintained, modified, or discontinued. We can hypothesize that MTX was reduced (modification or discontinuation group) when the patient’s condition had improved.
Table 5 Disease activity and participants’ physical function: evolution at 12 months and 24 monthsFrom the participants’ perspective, physical function improved at M12 and stabilised at M24, with mean changes (SD) from baseline in the adjusted HAQ-DI of − 0.3 (0.6) at both time points (Table 5). Up to 61 (48.4%) participants reported a clinically meaningful improvement in physical function.
Comments (0)