Transesophageal echocardiography to rapidly diagnose cardiac herniation following pneumonectomy
Purpose
To describe the use of transesophageal echocardiography (TEE) in the diagnosis of cardiac herniation following pneumonectomy, a serious complication that requires rapid recognition and management to prevent death.
Clinical features
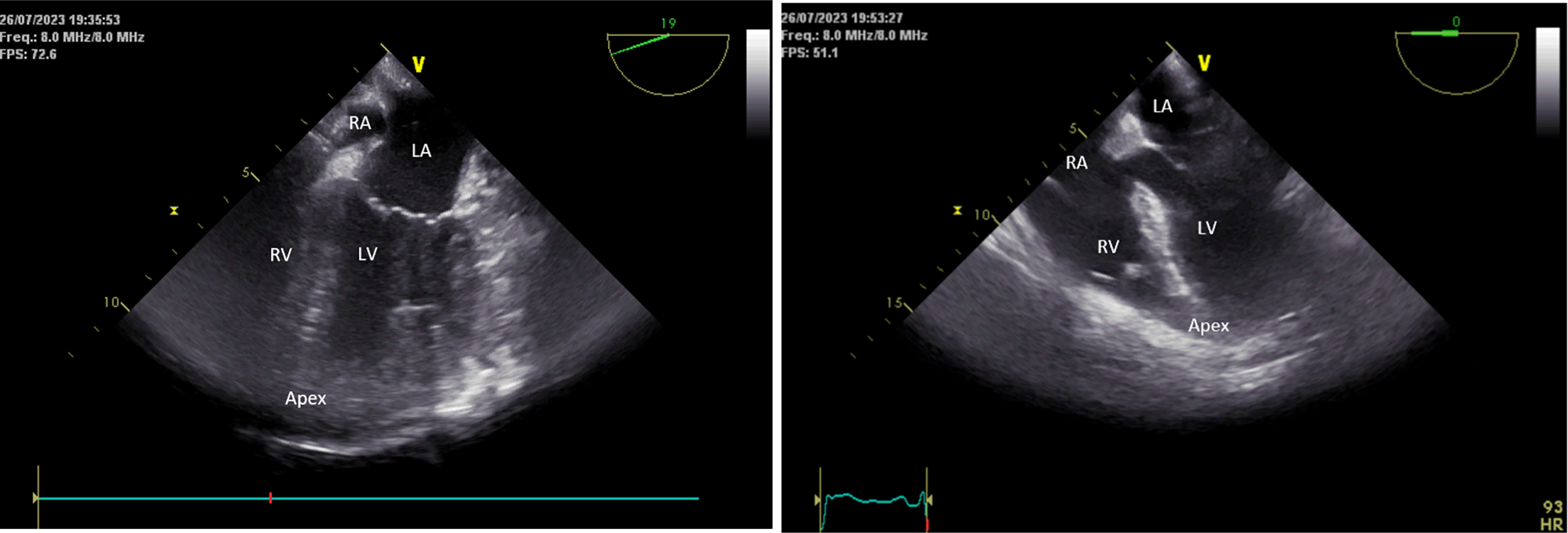
We present a case report of a 65-yr-old man referred for right intrapericardial pneumonectomy in the context of a right lower lobe lung cancer invading the hilum following induction targeted therapy. At the end of surgery, the patient’s trachea was successfully extubated and the vital signs were stable. On preparation to exit the operating room, the patient’s blood pressure (BP) suddenly dropped, and he became pale and unconscious. Chest compressions were rapidly initiated, and the patient’s trachea was reintubated. Return of spontaneous circulation was obtained after 3 min of resuscitation. A TEE probe was quickly inserted, and the examination showed hyperdynamic right and left ventricles with the apex of the heart oriented towards the right side of the patient instead of the usual left. In addition, the right atrium was partially collapsed, and a redundant wall and a mass effect were seen at the level of the interatrial septum. These images strongly suggested that the heart had twisted on its longitudinal axis, leading to a torsion of the superior vena cava, inferior vena cava, and right atrium—consistent with a cardiac strangulation or herniation. The surgical team reopened the patient urgently, the heart was repositioned in the pericardium, and the pericardial defect was closed with a GORE-TEX® patch. The postoperative course was uneventful.
Conclusions
Transesophageal echocardiography can be useful in diagnosing cardiac herniation following pneumonectomy.


Comments (0)