
Remember me

This study used a cross-sectional observational design, with participants undergoing endogenous pain modulation assessment at an initial testing session, followed by motor neurophysiological assessment at a subsequent session (within one week). A larger cohort underwent pain modulation assessment (Vallance et al. 2025a, b), while a smaller subset of these participants also completed motor neurophysiological testing (Vallance et al. 2024); here, we report findings for the smaller nested subset of participants for whom data from both assessments were available. Notably, when examining motor neurophysiological outcomes in our prior publication, we observed lower knee extension maximal voluntary isometric force (MVIF) compared to asymptomatic athletic controls (Vallance et al. 2024)–given the current study draws from that cohort, we proceed with the assumption participants included in this study demonstrate lower knee extension MVIF typical of individuals with patellar tendinopathy (Obst et al. 2024).
Our study was approved by the Monash University Human Ethics Committee (MUHEC project ID: 19892), and we collected written informed consent from all participants. We used both the Strengthening the Reporting of Observational Studies in Epidemiology recommendations for cross-sectional and case-control studies, and the International Scientific Tendinopathy Consensus (ICON) recommended standards, to guide reporting in this study (Rio et al. 2020).
SettingsParticipants attended two separate testing sessions, each for a duration of two hours. The first session took place at the Monash Exercise Neuroplasticity Unit research laboratory, located at Monash University Peninsula Campus, Victoria, Australia, or at a private physiotherapy clinic in Melbourne, Victoria, Australia, and focused on endogenous pain modulation assessment. The second session was conducted at the same research laboratory specified above and focused on motor neurophysiological assessment.
ParticipantsBetween June 2020 and January 2023, we recruited participants from Melbourne-based sub-elite and community-based basketball and volleyball organisations. Additionally, we utilised advertisements on social media, as well as within Monash University departments. We initially contacted individuals who expressed interest in participating in our study via a telephone call, during which screening questions were answered.
Individuals passing the initial telephone screen were subsequently invited to attend the initial assessment, where a physical examination was conducted by a trained physiotherapist (PV) to confirm their eligibility. Participants were included if they were a basketball or volleyball athlete aged 18 years or above who met specific criteria to confirm the clinical diagnosis of patellar tendinopathy. Specifically, this diagnosis was based on self-reported pain that was localised to the inferior pole of the patella, which could be confirmed in the physical examination via palpation of the corresponding site (Millar et al. 2021). Additionally, participants were required to report features consistent with patellar tendinopathy, including (i) a gradual onset of symptoms that had lasted three months or longer; (ii) aggravation of pain with activities considered to load the patellar tendon (e.g., running, jumping, and/or walking downstairs); and (iii) heightened intensity of pain following periods of inactivity, such as upon waking, or following prolonged periods of sitting.
Participants also performed a single leg decline squat (SLDS), and were required to report a pain rating of at least 2/10 on an 11-point numerical rating scale (NRS; with 0 = no pain, and 10 = the worst pain imaginable) at 90o knee flexion (Malliaras et al. 2015). Additionally, we used ultrasound imaging (Mindray M7, Shenzhen, China) to confirm the clinical diagnosis of patellar tendinopathy via detection of signs considered typical of tendinopathic change. These included hypoechoic regions within the proximal patellar tendon, and tendon thickening–notably, we employed a conservative threshold of >4 mm anterior-posterior diameter (Breda et al. 2021). This imaging was performed by an experienced physiotherapist, who is trained in the use of this technology (PV).
We excluded individuals if they were experiencing any painful condition at the time of testing (besides patellar tendon pain), or if they had experienced any painful condition within the prior six months to assessment that had lasted longer than one week, or that had been severe enough to require consultation with a health care professional. We also excluded individuals if they had received an injection (e.g., corticosteroid, platelet rich plasma or any other pharmaceutical agents) to the patellar tendon region or its surrounds within the six months prior, if they had a history of severe headaches or migraines, or had been diagnosed with type II diabetes, neurological conditions or an inherited connective tissue disorder. Further, we excluded anyone with metal in the cranial region, while all participants were also required to complete and fulfill the requirements of the TMS safety questionnaire (Rossi et al. 2011).
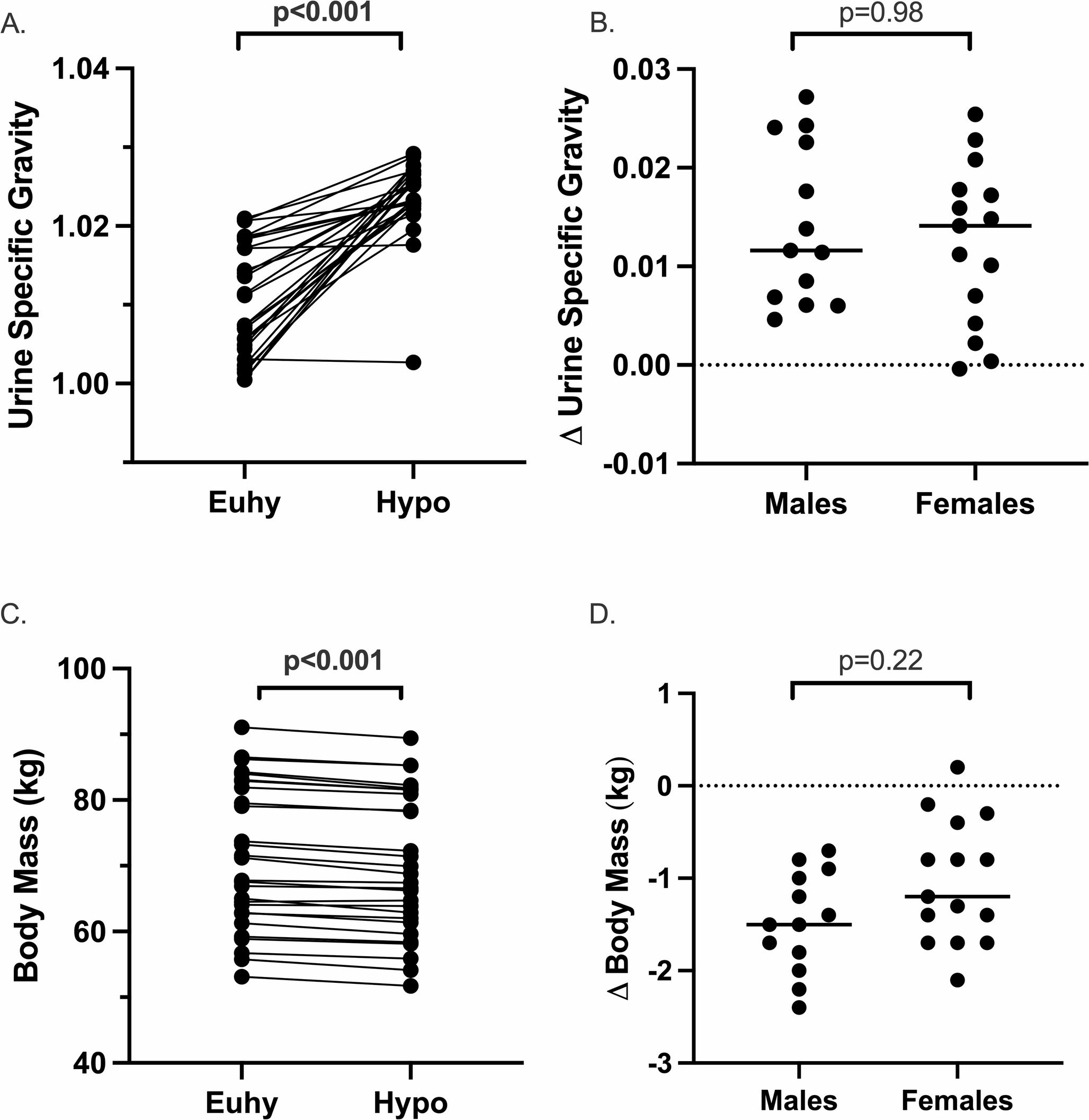
ProcedureAt the initial testing session, we collected demographic and tendinopathy-specific details (e.g., duration of symptoms), and participants completed the VISA-P questionnaire (0–100, where 100 indicates no patellar tendon pain or functional impairments) (Visentini et al., 1998). Following this, we assessed the efficacy of neural circuits responsible for endogenous pain inhibition and facilitation, using an approach we have described in detail in a prior publication (Vallance et al. 2025a, b). A summary of endogenous pain modulation assessment procedure, and the motor neurophysiological assessment completed in the subsequent session, is provided in Fig. 1.
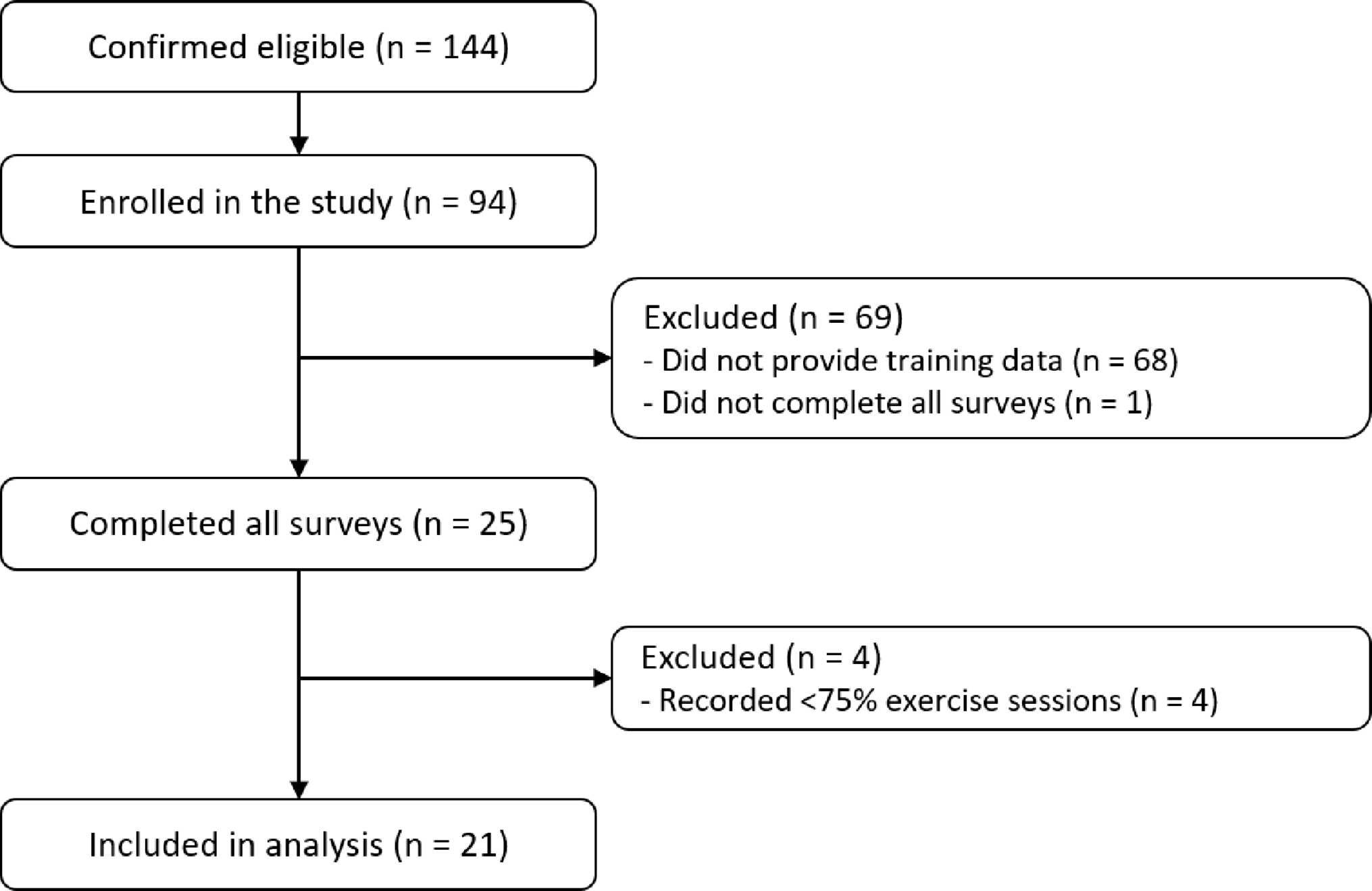
Fig. 1
Participant flow through the first (endogenous pain modulation assessment) and second session (motor neurophysiological assessment). PPT pressure pain threshold, NRS numerical rating scale, MVIF maximum voluntary isometric force, MMAX maximum compound action potential
Endogenous pain modulation assessmentWe utilised a conditioned pain modulation protocol consistent with our prior investigation (Vallance et al. 2021), that conformed to the recommended approach (Lewis et al. 2012; Pud et al. 2009). We collected pressure pain thresholds (PPT; Newtons [N]) with a digital algometer (Force One FDIX, Wagner Instruments, Greenwich, USA) over the most painful site on the affected/most affected patellar tendon, the ipsilateral-side tibialis anterior muscle belly, and contralateral side lateral elbow epicondyle, before and immediately after the ipsilateral side hand (i.e., opposite to the elbow used for PPT assessment) was submerged in water cooled to induce pain. Sites were assessed in a computer-generated randomised order. We submerged participants hand in this water for a total duration of 120 s, up to the level of the wrist crease with fingers spread wide to avoid laminar warming (Tompra et al. 2016), with water temperature starting at 8 °C.
We aimed to evoke a minimum pain response of 3/10 NRS within 20 s of the hand being submerged; if this rating was not met, we planned to reduce water temperature by adding ice until the minimum pain target was achieved (at which point, water temperature was maintained). Notably, this rating was met in all participants without the need to add further ice. We asked participants to rate their pain at their hand on the NRS at five, 20, 60 and 120 s (Chimenti et al. 2020). Endogenous pain inhibition was quantified as percentage (%) change in PPT from before to immediately after painful cold-water immersion, and endogenous pain facilitation as the change in hand pain on the NRS while immersed in water, from the fifth to the 20th second (Chimenti et al. 2020). Pain inhibition was calculated at all three sites (Murphy et al. 2021). A number of steps were undertaken to enhance the consistency of endogenous pain measurement at either test settings (private physiotherapy clinic or research laboratory); namely, the same digital algometer and cold-water apparatus were used for all endogenous pain assessments, and this was carried out by the same trained physiotherapist (PV).
As the site utilised to apply the painful conditioning stimuli in our protocol was remote to the injured patellar tendon, our interpretation of endogenous pain modulation outcomes focused on the influence of supraspinal mechanisms on these responses. Specifically, this includes enhanced projections from supraspinal centres to facilitate or inhibit the transmission of nociceptive afferents at the spinal cord dorsal horn (Yarnitsky et al. 2014). This is as opposed to
segment specific effects, such as activity of nociceptors local to the injured patellar tendon that – if sensitised – could alter afferent input to influence endogenous pain response. Insight for the activity of such local neural elements would require a conditioning stimulus be applied to the affected area instead, although a limitation to that approach is that it would not be possible to delineate the influence of segment-specific from supraspinal mechanisms on the resulting endogenous pain response (Yarnitsky et al. 2014).
Motor neurophysiological assessmentIn the second testing session, we assessed participants knee extension MVIF, before measuring the excitability of neural elements that influence force production (i.e., motor neurophysiological outcomes). Our approach for this assessment has been described in detail in a prior publication (Vallance et al. 2024). Briefly, participants sat in our custom designed chair throughout this assessment, with their hips flexed to 90o and their affected/most affected knee flexed to 60o. We attached the affected/most affected limb to an S-Type load cell (Sparkfun, Niwot, Colorado, USA) which had been calibrated to known values at the inferior tibia region – we attached the opposite end of the load cell to our chair, enabling knee extension force to be resisted isometrically.
Prior to electrode placement, we shaved the designated site to remove fine hair, applied an abrasive gel to remove dead skin cells, and sanitised the area using 70% isopropyl alcohol. We subsequently placed bipolar Ag–AgCl electrodes on the rectus femoris muscle to collect surface electromyography (sEMG), consistent with SENIAM guidelines (Hermens et al. 2000). We sampled and captured force signal (2048 Hz) using PowerLab 4/26, with a connected single-channel bridge amplifier (ADInstruments; Bella Vista, Australia) to allow force recordings to be synchronised with measures of neural element excitability. We amplified sEMG signal by the factor of 1000, and applied high- (13 Hz) and low-bandpass filtering (1000 Hz). Following collection, we analysed all signal recordings using PowerLab 4/26 software (ADInstruments, Bella Vista, Australia).
Following a familiarisation trial, participants performed two recorded knee extension maximal voluntary isometric force (MVIF) trials on their affected limb, interspersed with a rest period of at least 30 s. If maximal force achieved in these two trials differed by more than 5%, additional trial/s were performed until two trials were within this threshold (one of which being the highest force achieved). We considered the peak knee extension force achieved across all recorded trials to be the knee extension MVIF, and present this in its natural unit format (Kg/f) as well as standardised to body weight (Kg/Kg).
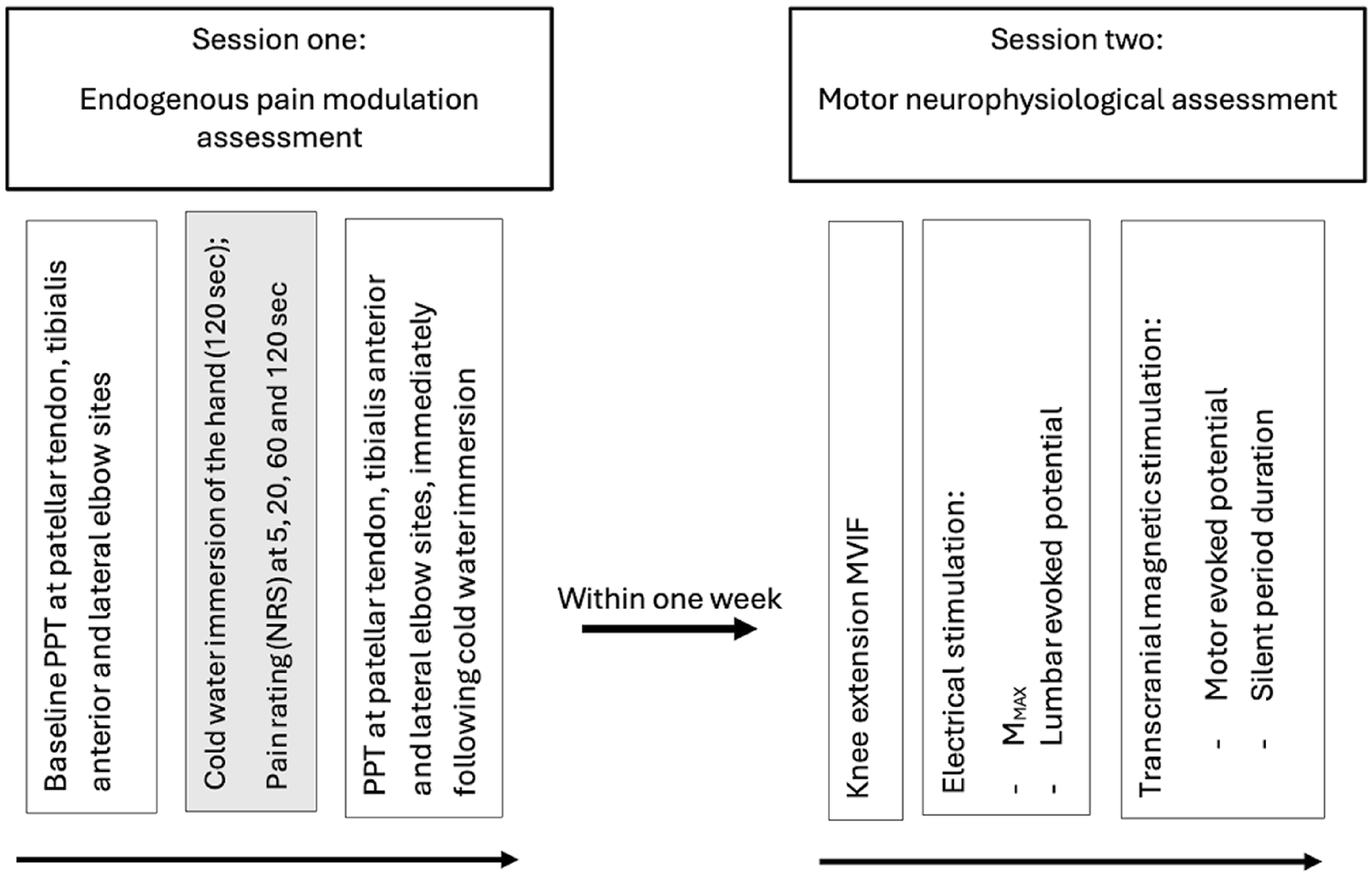
We used a range of electrical stimulation and transcranial magnetic stimulation (TMS) techniques to assess the excitability of neural elements that contribute to knee extension motor output (Fig. 2). To apply electrical stimulation, we used a constant-current device (Digitimer DS7AH). Specifically, we assessed maximum compound action potential (MMAX) by delivering supramaximal electrical stimuli to the femoral nerve, and considered the highest peak-to-peak sEMG evoked with this approach to indicate the maximum muscle response (Rodriguez-Falces and Place 2018). We also used electrical stimulation to assess lumbar evoked potentials (LEPs), via application to the spinous processes of the first lumbar vertebra and eighth thoracic vertebra. We defined LEP as the electrical stimulation output (ESO; in mA) required to achieve sEMG amplitude within 5–10% of the MMAX (Škarabot et al. 2019a, b). As LEP is considered to reflect the efficacy of efferent transmission between the corticospinal tract neurons and motoneurons (Škarabot et al. 2019a, b), a higher LEP ESO corresponds with lower spinal excitability (Vallance et al. 2024).
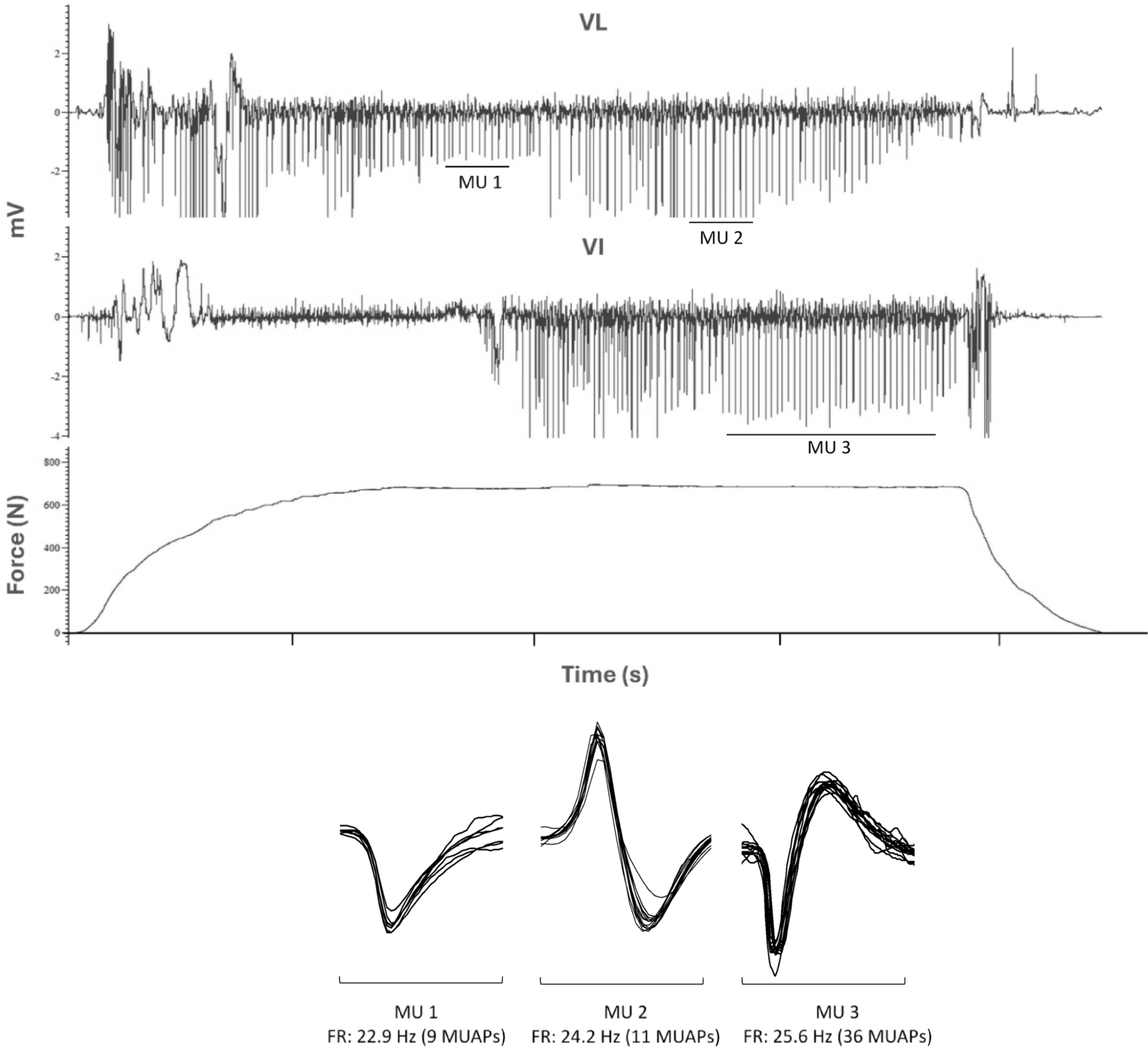
Fig. 2
Visual representation of surface electromyographic (sEMG) data analysed, including A motor evoked potential (MEP; peak-to-peak sEMG following transcranial magnetic stimuli at 130% of active motor threshold, normalised to maximum compound action potential amplitude) and silent period duration (measured from onset of motor evoked potential to resumption of voluntary sEMG drive, and B maximum compound action potential (MMAX; peak-to-peak sEMG following electrical stimuli at a supramaximal intensity applied to the femoral nerve) and lumbar evoked potential (LEP; recorded as the electrical stimulator output required to elicit peak-to-peak sEMG equivalent to 5–10% of MMAX sEMG, applied to the lumbar region). mV millivolts, ms milliseconds
We used a Magstim 2002 device (Magstim Co., Ltd, Whitland, UK) to apply TMS, which was consistently administered over the M1 ‘hotspot‘ (Rothwell et al. 1999) while participants maintained 20% MVIC knee extension force. Notably, this hotpot was marked with a non-permanent marker to enable accurate application of stimuli. We delivered single-pulse TMS at 130% of active motor threshold to produce motor evoked potentials (MEP), which we calculated as the average peak-to-peak amplitude (mV) across 10 trials, expressed as a proportion of MMAX. Higher MEP amplitude is widely considered to indicate greater corticospinal excitability (Vallance et al. 2025a, b). We also calculated the period of sEMG inactivity following each single-pulse TMS-evoked MEP, which is recognised as the silent period. Specifically, we measured from the onset of the MEP to the reactivation of voluntary sEMG activity. The silent period is a marker of corticospinal inhibition, mediated by gamma-aminobutyric acid-B (GABA-B) receptor activity (Škarabot et al. 2019a, b).
Statistical analysisAs this is a secondary analysis study, participants were enrolled to satisfy the requirements of our prior publication (Vallance et al. 2024). All analysis was completed using Statistical Package for the Social Sciences (SPSS; v.29; Chicago, USA). We inspected each outcome for normality using the Shapiro-Wilk test, and visual inspection of Q-Q plots. We present non-normally distributed data as median (interquartile range), and normally distributed data as mean (standard deviation). For correlational analysis, if one or both variables included were non-gaussian, we used Spearman’s Rho, while Pearson’s correlation coefficient was used if both variables being analysed were normally distributed. We investigated if endogenous pain facilitation or endogenous pain inhibition at the patellar tendon site shared association with motor neurophysiological outcomes (LEP ESO, MEP or silent period duration), or knee extension MVIF. Additionally, we investigated if symptom duration was association with any of these motor neurophysiological outcomes. To guide interpretation of correlations, 0.00–0.09 was considered the absence of a correlation, 0.10–0.39 a weak correlation, 0.40–0.69 moderate, 0.70–0.89 strong, and 0.90–1.00 a very strong correlation (Schober et al. 2018). Where any data were missing, cases were excluded from correlational analysis pairwise. To control for multiplicity, p values were adjusted using the Benjamini–Hochberg method as this approach is considered appropriate for exploratory analysis (Benjamini et al. 2001; Benjamini and Hochberg 1995).
To reduce the number of comparisons performed, we only included endogenous pain inhibition at the patellar tendon site in correlational analyses. To ensure this selection did not influence results, we performed sensitivity analysis to confirm the inclusion of pain inhibition response at the tibialis anterior or lateral elbow sites in correlations would not have produced different outcomes. Moreover, for identical reasoning, we only included knee extension MVIF in its raw unit in correlational analysis, so we performed sensitivity analysis to confirm inclusion of MVIF normalised to body weight (Kg/Kg) instead would not have influence results. Multiple comparisons were calculated for corresponding sensitivity analyses to enable fair comparison. We also tested the assumption that endogenous pain inhibition or facilitation response was not related to the intensity of hand pain experienced at five seconds immersion via correlational analysis, to ensure conclusions drawn for supraspinal influence on pain modulation (as opposed to peripheral input) were sound.
We used simple linear regression to examine the association between endogenous pain and motor neurophysiological outcomes, or knee extension MVIF, based on correlational analysis results (threshold for inclusion in models, p < 0.010). Where data were missing, we utilised group mean. Based on our modest sample and potential departures from normality, we incorporated bootstrapped regression coefficients and report bias-corrected and accelerated (BCa) confidence intervals (4000 resamples, with a fixed random seed for reproducibility; simple sampling method) (LaFlair et al. 2015). Holm-Bonferroni corrections were applied to p values associated with BCa intervals to control for multiple comparisons.
Residual plots were produced and visually inspected to check model assumptions were satisfied. Additionally, we computed diagnostics (Cook’s distance [D]) to assess for potential individual case leverage (indicated by Cook’s D > 1.0) and for sensitivity analysis – we re-ran each model after removing the observation with the highest Cook’s distance to determine potential influence of leverage; effect estimates and BCa intervals were compared to original models for stability. The significance for analysis associated with regression analysis was also set to p < 0.05.
Comments (0)