
Remember me
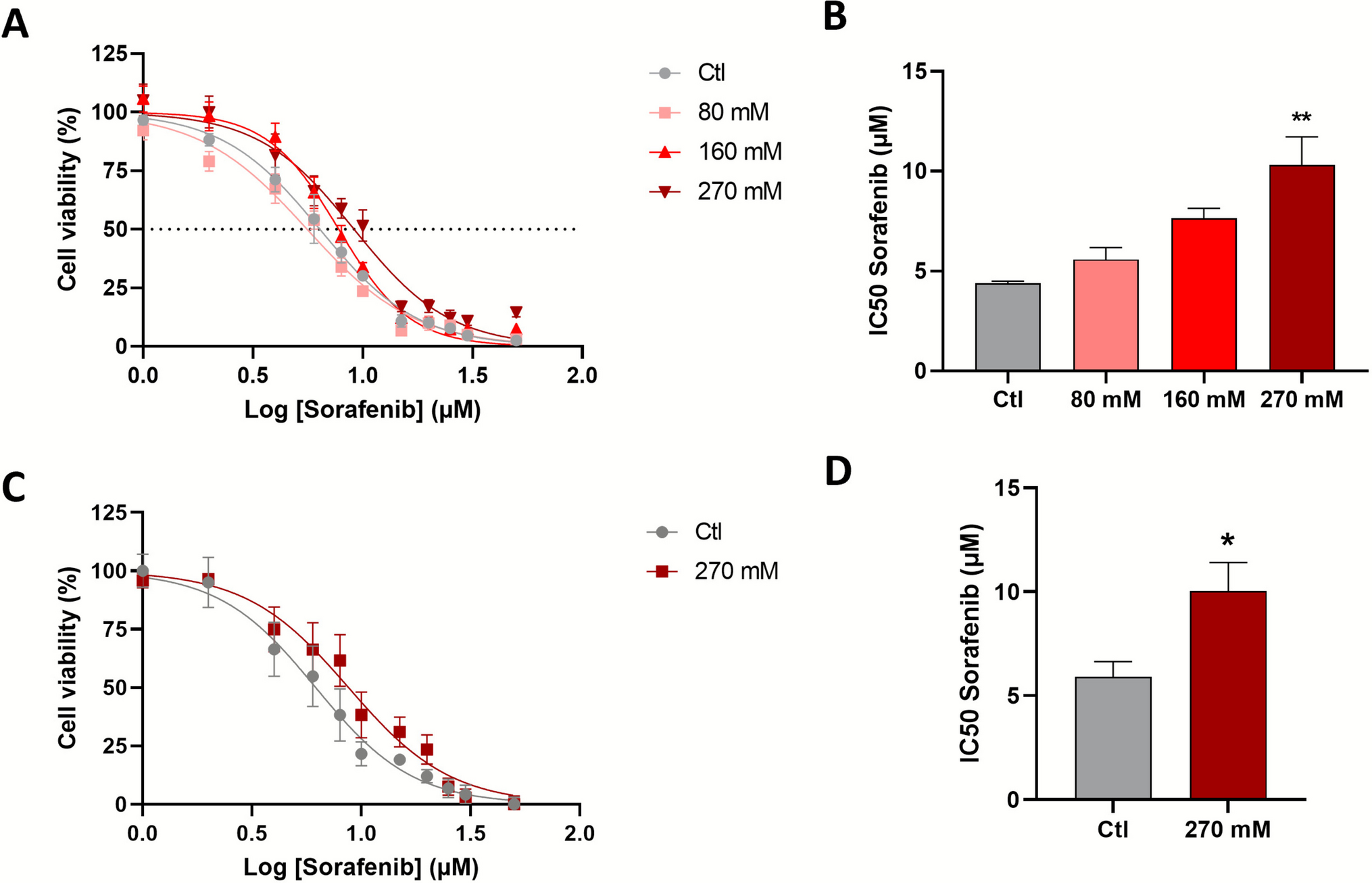

First, in order to determine the effect of CAE on sorafenib sensitivity, we determined the IC50 of sorafenib in Huh-7 cells. Cells were cultured following the CAE protocol, with a 6-month alcohol exposure at different concentrations: 80 mM, 160 mM, and 270 mM. The results show an alcohol dose-dependent shift to the right of the cell viability curve. Compared to the control (Ctl) cells, 270 mM CAE cells exposed to sorafenib had more viability (Fig. 1A). Then, for the Ctl condition, the IC50 was 4.4 ± 0.09 µM. There was a non-significant increase in the IC50 of sorafenib for the 80 and 160 mM conditions compared with control cells (p = 0.187 and p = 1.00, respectively). There was a statistically significant increase in IC50 with CAE at 270 mM, reaching a value of 10.3 ± 1.4 µM (p = 0.006, Dunn’s test) (Fig. 1B). An increase of 134.1% compared with Ctl cells. These results highlight a decrease in the sensitivity to sorafenib, reflecting the acquisition of CAE cell resistance.
Fig. 1
Chronic alcohol exposure induces an increase in the resistance of Huh-7 cells to sorafenib. The cell viability of Huh-7 cells treated with sorafenib concentrations (0–50 µM) was studied using MTT (A) and cell titer (C) assays, which allowed the determination of sorafenib IC50 (B and D). The MTT and cell titer assays were performed 72 h after sorafenib treatment. Results were pooled from four independent experiments and the corresponding mean ± SEM of sorafenib IC50 is presented in (B) and (D). The Kruskal–Wallis test and Dunn’s post hoc test were used for the MTT assay (N = 4; **p < 0.01 vs. Ctl). Student’s t-test was employed for the cell titer assay (N = 6; *p < 0.05 vs. Ctl)
With regard to the results of the cell titer assay, for the control condition, the IC50 was 5.92 ± 1.7 µM. Alcohol exposure induced a shift of the cell viability curve to the right, and an increase in IC50 was observed at 270 mM, reaching 10.03 ± 3.4 µM (Fig. 1D). This increase was statistically significant (p = 0.025, student’s t-test).
We also studied the effect of CAE on the response to lenvatinib, another first-line tyrosine kinase inhibitor treatment for advanced HCC. We observed an increase in the IC50 of lenvatinib at the 160 mM condition compared with the control condition (p = 0.019), but not at 270 mM (p = 0.768) (Suppl Fig. 1 A and 1B). This absence of a dose-dependent trend was unexpected and may reflect non-linear cellular responses at high ethanol levels. Secondly, we looked at second-line TKI treatments for patients with advanced HCC, namely regorafenib and cabozantinib. The results showed a dose-dependent rightward shift in cell viability (Suppl Fig. 1 C and 1E). We observed an increase in the IC50 of regorafenib and cabozantinib with CAE at 270 mM (Suppl Fig. 1D and 1 F). This was significant for cabozantinib (p = 0.033) but not for regorafenib (p = 0.152). These results highlight a decrease in sensitivity to regorafenib and cabozantinib with CAE, reflecting the acquisition of cellular resistance. Our results demonstrate the acquisition of resistance to different targeted therapies following exposure to alcohol.
CAE activates ERK signaling pathways in Huh-7 cells treated with sorafenibWe investigated the impact of CAE on the signaling pathways involved in sorafenib resistance with Western Blot experiments. In Ctl cells not exposed to ethanol, we observed a significant decrease in mTOR phosphorylation with sorafenib at 5 µM (0.434-fold, p = 0.004) and 10 µM (0.526-fold, p = 0.013) compared to non-sorafenib treated Ctl cells. Our experiments demonstrated also a significant decrease of ERK 1/2 phosphorylation in Ctl cells with sorafenib at 10 µM (0.41-fold, p = 0.025) compared to non-sorafenib treated Ctl cells. Sorafenib at 5 µM and 10 µM in CAE 270 mM had no effect on mTOR and ERK1/2 phosphorylation. Sorafenib treatment did not modify the expression of Ras protein in Ctl and CAE 270 mM cells (Fig. 2A and B). These results are schematically summarized in Fig. 2C.
Fig. 2
Chronic alcohol exposure modifies signaling pathways implicated in sorafenib response. Protein expression was analyzed by Western blot in Huh-7 cells. GAPDH, mTOR (Ser2448), Ras, and ERK1/2 (Thr202/Tyr204) were used as controls (N = 4). Results were pooled from four independent experiments, and their corresponding mean ± SEM of protein activation and expression levels are presented (A). One of the four independent experiments is presented in (B). Results were simplified in the schematic (C). RTK, receptor tyrosine kinases
Efflux transporters are not involved in the acquisition of sorafenib resistance induced by CAESeveral studies have demonstrated the involvement of efflux transporters in treatment resistance in HCC. Therefore, we wanted to study the impact of CAE on efflux transporter activity. To do this, we studied the effect of CAE on the accumulation of rhodamine123 (R123) in Huh-7 cells. After cell recovery and fluorescence analysis by flow cytometry, we observed a slightly lower retention of R123 in alcohol-treated Huh-7 cells (Suppl Fig. 2 A). These results suggest higher efflux transporter activity at 160 mM and 270 mM alcohol in Huh-7 cells compared with the 80 mM condition (p = 0.004 and p = 0.003, respectively). However, there was no significant difference compared with the control condition.
To confirm this result, we assessed the expression of various efflux transporters of the ABC family, known to be involved in this mechanism of resistance. Our results show a significant increase in the expression of ABBC1 (MRP1) transcripts in 270 mM CAE cells (p = 0.049). No difference in ABCB1 (MDR1) transcript expression was induced by CAE (p = 0.99). Surprisingly, CAE caused a significant decrease in the expression of ABCG2 transcripts (p = 0.006, Suppl Fig. 2B). We then studied the protein expression of the MRP1 and MDR1 transporters by flow cytometry, and CAE did not modulate their protein expression (Suppl Fig. 2 C). Subsequently, we used the EFFLUX-ID Gold kit (Enzo Life Sciences) to specifically determine the activity of the MRP1/MRP2/MRP3, MDR1, and ABCG2 transporters, using inhibitors, following the manufacturer’s instructions. We did not observe a significant difference with alcohol exposure in the activity of the efflux transporters MRP, MDR1, and ABCG2 (p = 0.12, p = 0.81, p = 0.11 respectively, ANOVA, Suppl Fig. 2D).
Identification by RNAseq of differentially expressed and drug resistance-related genes induced by alcoholIn order to determine the mechanisms of resistance to treatments induced by alcohol exposure, we conducted RNA Sequencing on our Huh-7 control cells and 270 mM CAE cells (Fig. 3).
Fig. 3
Differentially expressed genes and pathways associated with CAE in huh-7 HCC cells. A Venn diagram of the number of expressed genes between control Huh-7 cells and EtOH huh-7 cells. B Volcano plot of differentially expressed genes obtained by RNA-seq. Genes with a log2 fold change ≤ − 1 are considered downregulated, while those with a log2 fold change ≥ 1 are considered upregulated. The horizontal threshold corresponds to statistical significance based on adjusted q-values. C KEGG pathway classification. The vertical axis represents the pathway. The horizontal axis is the enrichment ratio. The size of the bubble represents the number of genes annotated to KEGG Pathway. The color represents the enriched significance with the specific q-value. The q-value was obtained by the correction of the p-value (q-value < 0.05 is considered as significant enrichment) (EtOH/Ctl). D Heat map expression levels of 80 drug resistance genes obtained by RNA sequencing
Based on the Venn diagrams, we identified 16,261 common genes between our two conditions (Fig. 3A). Additionally, 408 genes are specific to the Ctrl condition, while 786 genes are specific to the 270 mM condition. Among the 16,261 genes, we further extracted 1405 differentially expressed genes and visualized them in the volcano map (Fig. 3B), including 815 upregulated and 590 downregulated genes. The results of the KEGG (Kyoto Encyclopedia of Genes and Genomes) pathway enrichment analysis showed 20 differentially expressed pathways in Ctrl and 270 mM cells (Fig. 3C). We obtained a list of drug resistance and aggressiveness genes from the KEGG pathway. A total of 80 genes were retrieved for drug resistance and are depicted in the heat map, such as genes involved in angiogenesis (VEGF, PDFGA/B/D). We also find the MRAS (log2270mM/Ctl = 3.09), PROM1 (CD133) (log2270mM/Ctl = 3.15), and CD36 genes (log2270mM/Ctl = 3.07) (Fig. 3D). These genes showed significant differential expression between Ctrl and 270 mM cells. These results show significant differences in the transcriptomic profiles of HCC cells chronically exposed to alcohol or not.
Alcohol-related HCC patients are less responsive to sorafenibA total of 86 patients with HCC were enrolled in this study, including 54 patients in the alcohol-related HCC group and 32 patients in the non-alcohol-related HCC group. The baseline characteristics of the patients are shown in Table 1.
Table 1 Baseline characteristics of HCC patients according to alcohol consumptionThe gender distribution is significantly different between our two groups (p = 0.004). There were 53 (98%) men and 1 (1.9%) woman in the alcohol HCC group and 25 (78%) men and 7 (22%) women in the non-alcohol HCC group. No clinically relevant differences were observed between the groups in terms of median age at the time of inclusion or biochemical characteristics (AST, ALT, alpha-fetoprotein, bilirubin, creatinine, albumin, and prothrombin) at the time of sorafenib treatment.
The BCLC stage was assessed in 57 (66.3%) patients (information was missing for 29 (33.7%) patients). The distribution of BCLC stages between alcohol and non-alcohol groups did not significantly differ (p = 0.4). However, the Child–Pugh liver function class differed between the two groups (p = 0.013). In the HCC alcohol group, 39 (91%) patients had a Child A score, and 4 (9.3%) had a B score. In the non-alcohol HCC group, 17 (65%) patients had a Child A score, and 9 (35%) had a B score.
We subsequently evaluated the response to sorafenib, taking into account the etiology of HCC, whether alcohol-related or non-alcohol-related. Patients with alcohol-related HCC had a significantly lower response rate to sorafenib compared with patients with non-alcohol-related HCC (35% (n = 19) versus 63% (n = 20) respectively, p = 0.014).
Alcohol reduces overall survival (OS) and increases HCC progression in HCC patients treated with sorafenibBefore conducting the multivariate analysis, variables were balanced using the method of SMD (Suppl Fig. 3). The median OS was 10 months (95% CI = [6.1, 15.7]) and 12.1 months (95% CI = [7.7, 64.9]) in the “Alcohol” and “Other etiology” groups, respectively (Fig. 4A). Alcohol-related HCC significantly shortened the lifespan of patients (p = 0.0234). The proportions of patients at risk of death at 36 months were 4% and 30% in the respective groups.
Fig. 4
Alcohol consumption decreases survival of patients with hepatocellular carcinoma treated by sorafenib. The overall survival (OS) (A) and progression-free survival (PFS) (B) of 86 HCC patients were presented as Kaplan–Meier curves and compared using the log-rank test. The number of patients at risk was listed below the survival curves
The median progression-free survival (PFS) was 5.72 months (95% CI = [4.63, 12.8]) in the alcohol-related HCC group versus 9.66 months (95% CI = [4.40, 39.9]) in the non-alcohol-related HCC group (Fig. 4B). Alcohol-related HCC patients had significantly shorter PFS (p = 0.0298). The proportions of patients without progression or at risk of death at 18 months were 11% and 41% in the respective groups. Both OS and PFS were better in the non-alcohol-related HCC group.
Comments (0)