GLIM criteria: from consensus to practice in inflammatory bowel disease
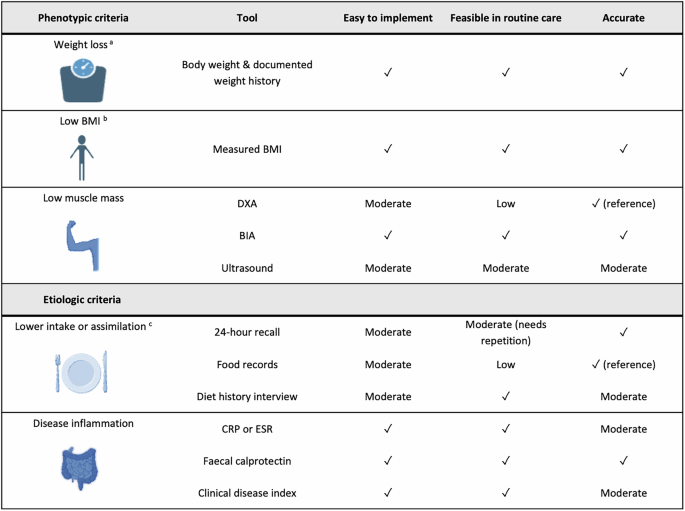
The Global Leadership Initiative on Malnutrition (GLIM) criteria were developed to provide a practical, simplified, and uniform malnutrition diagnostic framework that could be implemented consistently across different clinical settings and patient populations [1]. However, Bletsa et al. demonstrated substantial variability in how the GLIM criteria has been implemented in inflammatory bowel diseases (IBD) studies. Much of this heterogeneity stems from the wide range of tools and cut-offs used to assess both phenotypic and aetiologic criteria [2]. This inconsistency not only limits comparability between studies but also weakens the clinical utility of the GLIM framework in IBD. To address this challenge, there is a pressing need to highlight assessment tools that strike a balance between ease of implementation (in terms of low burden and training requirements), feasibility (low cost and ready access), and high accuracy for each component of the GLIM criteria in patients with IBD. As the recently published ECCO consensus recommends that every newly diagnosed patient with IBD and those at risk of malnutrition should undergo a nutritional assessment [3], it is essential to consider these factors in real-world practice, highlighting the need for a consistent approach applicable across diverse clinical settings.
Malnutrition according to the GLIM is defined by at least one phenotypic criterion and one aetiologic criterion. The three phenotypic criteria are nonvolitional weight loss, low body mass index (BMI), and low muscle mass. The former two are the easiest to implement and therefore, commonly reported, yet definitions and cut-offs varied considerably across studies. Weight loss remains the most accessible and clinically meaningful GLIM parameter, and prioritisation should be given to objectively documented, serial body-weight measurements obtained from medical records. When unavailable, patient-reported weight history may be used. Importantly, weight loss should be interpreted alongside BMI, as BMI alone has well-known limitations in detecting malnutrition, as it does not account for body composition or accurately reflect muscle mass [1].








Comments (0)