
Remember me
In managing RVF in the MICU, priority should be given to addressing potentially reversible causes. This includes minimizing the use of common ICU medications and treatments that may exacerbate RVF, such as alpha-agonists, negative inotropes, and hypotension-causing agents like Dexmedetomidine. After mitigating reversible etiologies, the treatment strategy for acute RVF in critically ill patients should focus on three core mechanisms: (1) optimizing RV preload to reduce excessive volume and prevent RV dilation; (2) Reducing afterload to alleviate RV strain; and (3) enhancing contractility to improve RV function.
RV Preload OptimizationVolume maintenance is one of the most impactful ways to improve hemodynamics in RVF. RV dilation results in anatomical distortions leading to decreased contractility of the RV itself and shifting the IVS leftward, thereby decreasing LV size and CO. A simple strategy to implement early in the course is intravenous fluids (IVF) stewardship with special attention given to stopping continuous IVFs and increasing the concentration of pharmacotherapeutics. While there has been a traditional teaching that acute RVF should be treated first with a trial of small IVF bolus [22], this practice should be reserved for patients with clear evidence of hypovolemia, septic shock or acute RV infarction, where insufficient preload leads to decreased RV output. Studies have shown that volume loading patients with increased PVR results in a counter effect of decreased LV diastolic volume [83]. In hypervolemic patients, improved perfusion can be achieved with vasopressors and inotropy while avoiding the adverse effects of increased preload and deterioration into a detrimental spiral.
DiureticsAcute RVF often results in decreased renal blood flow leading to neurohormonal activation of the renin–angiotensin–aldosterone system (RAAS). This leads to increased sodium reabsorption, contributing to increased water reabsorption and loop diuretic resistance. The use of an early aggressive diuresis strategy is imperative for successful RVF treatment, as inadequate diuresis is associated with worse outcomes in acute decompensated HF patients with fluid overload. While diuresis is one of the most important treatments for RVF; it is important to view it also as a preventive measure against further deterioration.
There is robust evidence from multiple clinical trials, observational studies and meta-analyses consistently demonstrating that inadequate diuresis is associated with worse outcomes including increased mortality [84,85,86,87]. It is advisable to initiate treatment with high-dose loop diuretics to exceed the diuretic threshold, particularly in patients with decreased creatinine clearance (CrCl), who require higher doses to achieve adequate diuretic concentrations at the site of action [88, 89]. In the case of Furosemide, increasing the diuresis effect can be achieved by more frequent dosing every six hours once the diuretic threshold is established, as further dose escalation does not enhance the effect. Bolus dosing is preferred over continuous loop diuretic infusion due to its higher likelihood of reaching the diuretic threshold faster. Dosing should consider diuretic naivety, home dose, and available data such as spot urine sodium (UNa) or urine output (UOP) since presentation. A baseline spot UNa before diuretic administration can guide dosing and additional testing can be used to assess response, with UNa < 50 mmol/L indicating inadequate response, requiring dose increase [90]. In a prospective cohort study acute HF patients with low UNa excretion in the first six hours after initiation of loop diuretic therapy were found to have lower UOP and higher all-cause mortality [91]. It can be argued that spot Una is a more valuable parameter than UOP for assessing diuresis, as it provides earlier insights into diuretic response, enabling clinicians to adjust treatment regimens more rapidly during critical periods.
Diuresis TargetsIn severe acute RVF, diuresis targets should aim for 100–150 mL/hour (2–3 L/day) not to exceed 150 mL/hour to balance efficacy and safety, and CVP < 8 cm H2O [2, 37, 85, 90]. CVP reduction is associated with higher CO and improves 28-day prognosis in patients with circulatory shock [92]. The routine monitoring of daily weights and strict Ins and Outs has been one of the cornerstones of diuretic treatment response monitoring; however, recent studies found those to be poor measures due to being inaccurate and challenging to obtain in a timely fashion [93]. It is advisable to assess UOP goal and electrolytes every six hours in the initial 24 h, then every 12 h or assess natriuresis with spot urine sodium targeting goal of > 50–70 mmol/L after 2 h from diuretic regimen initiation [89]. It is not advisable to use oral diuretics given the high likelihood of decreased GI reabsorption from hypoperfusion or congestion of splanchnic circulation [94]. In patients with diuretic resistance and hypoproteinemia (from cardiointestinal syndrome), some studies suggest that coadministration of albumin can be beneficial [95].
Close monitoring of diuresis response, through hourly UOP recording or spot UNa, is essential for achieving negative fluid balance in a timely manner. A recent meta-analysis showed that high UNa after diuretic administration is associated with higher UOP, shorter hospital stays, and lower mortality odds [96]. The ENACT-HF study, a prospective, open-label trial, demonstrated that a protocolized diuresis regimen-guided natriuresis was superior to each institution’s standard of care. Patients on a diuresis protocol were found to have 64% higher natriuresis in the first day of treatment with sustained higher natriuresis and diuresis in the first two days, as well as one day shorter length of stay. The difference was even greater for patients with GFR < 49 or on prior high oral loop diuretic maintenance regimen [97]. The presence of systemic hypotension should not deter aggressive diuresis in hypervolemic patients; vasopressors can temporarily support systemic perfusion until RV hemodynamics improve. The widespread assumption that elevated creatinine and AKI invariably indicate tubular injury should be reconsidered, as multiple studies suggest this is not the case, but merely a reduction in GFR [98]. Studies like DOSE have shown that higher doses (e.g., 2.5 × home dose, up to 100 mg) are safe and efficacious [84], while other studies evaluating kidney function post-diuresis in patients with elevated CrCl further support these strategies. Ahmad et al. showed that while patients receiving high-dose loop diuretics experienced mild to moderate decrease in eGFR, this was not associated with elevations of tubular injury biomarkers, increased mortality or rehospitalization and possibly contributed to premature cessation of decongestive treatment. Another noted result was that changes in metrics of diuresis such as UOP and UNa were not linked to measures of kidney function such as creatinine and cystatin-C [99]. Further, in patients with Intra-abdominal pressure (IAP) > 8 mmHg diuresis also helps improving kidney function via decreasing abdominal hypertension [100]. Intraabdominal hypertension develops when IAP exceeds 8 mmHg and results in further organ dysfunction and most importantly decreased renal function, especially in patients who develop compartment syndrome. In patients with severe IAP, it is advisable to perform routine measurement of IAP via bladder pressure and paracentesis for frank ascites to improve kidney function [101]. In refractory cases, surgical management may be necessary.
Adjunctive TherapyPatients with diuretic resistance, severe volume overload and electrolyte derangements are likely to benefit greatly from combination diuretic therapy. While minimizing electrolytes disturbances is important, the removal of high volume of fluid expediently is of most importance in the initial stages of RVF treatment; therefore, the combination therapy contributing most to that should be preferred, while monitoring electrolyte levels closely.
In cases of severe RVF, non-respondents and cases where cardiorenal syndrome is suspected, early initiation of distal diuretics treatment is advised. A distal diuretic such as a thiazide, can be used in patients with suspected loop diuretic resistance-induced epithelial cell or distal tubular hypertrophy from chronic loop diuretic use [102]. In patients with hyperkalemia, initiation of thiazide or aldosterone antagonists such as Amiloride or Spironolactone may increase diuresis yield.
Although the ADVOR trial enrolled predominantly left-sided or biventricular heart failure, Acetazolamide, a carbonic anhydrase inhibitor (CAI) that blocks the proximal convoluted tubular absorption of sodium, in combination with loop diuretics, has emerged as an effective component of sequential nephron blockade in diuretic-resistant congestion [103]. CAIs should be used in cases of hypochloremic metabolic alkalosis, which may result from aggressive diuresis. However, given that most severe RVF patients are acidemic, caution should be used as CAIs cause normal AGMA.
Sodium bicarbonate enhances diuretic responsiveness by urine alkalinization and correcting metabolic acidosis, thereby improving myocardial contractility and catecholamine responsiveness. However, the high sodium load associated with its administration may increase fluid retention and adversely affect RV preload. Additionally, in patients with concurrent respiratory failure, it may exacerbate hypercapnia by increasing CO2 production, potentially leading to an increase in PVR.
UltrafiltrationEarly ultrafiltration (UF) for volume optimization can be significantly beneficial to RVF patients with volume overload, low urine output, and inadequate response to diuretics. While resource-intensive, prompt recognition and commitment to initiation of UF is essential for successful treatment, preventing a downward spiral that becomes challenging to reverse once established. In cases of severe interstitial edema, UF proves more efficient as it allows for the removal of more sodium for the same amount of fluid compared to diuretics [104]. In severe cases, it is advisable to initiate early UF within six hours of determining an inadequate response to a high-dose combination diuretic regimen or failure to achieve net negative fluid balance within the first 24 h of diuresis. As with diuresis targets, the UF goal target of optimal fluid status should be guided by CVP. CVP should be reduced to below 15 mmHg (goal 8–12 mmHg), while avoiding hypovolemia. Caution should be exercised in preload dependent patients, as rapid fluid removal can reduce venous return and result in a decrease in cardiac output. Therefore, avoidance of excessive UF rates (> 200–300 mL/h) is advised in the early stages with titration up as tolerated. It is often beneficial to temporarily withhold or drastically reduce loop diuretic therapy for 48–72 h during active UF, to interrupt the adaptive mechanisms of diuretic resistance, thereby restoring diuretic responsiveness once UF is stopped [105].
RV Afterload ReductionWhile preload management is important in preventing devolvement into a vicious cycle, reducing RV afterload can lead to rapid and dramatic improvement in RV function. Elevated afterload, frequently encountered in patients with preexisting pulmonary vascular diseases, can be treated by lowering pulmonary pressures through thrombectomy, thrombolysis, correction of acidosis, hypoxia and hypercapnia via optimizing ventilation, and decreasing lung congestion through diuresis. In this group, selective pulmonary vasodilators such as inhaled nitric oxide (iNO) and prostacyclin analogs allow for PVR reduction without causing systemic hypotension or worsening VQ mismatch [106]. It has been shown that iNO can enhance RVEF, reduce end diastolic volume, and improve pulmonary hemodynamics and oxygenation in RVF patients [107, 108]. In patients with RVF driven by left-sided heart failure with adequate blood pressure, decreasing LV afterload with systemic vasodilators may also reduce PVR and expedite the achievement of diuresis goals by improving renal perfusion and reducing preload. However, caution should be used when using pulmonary vasodilators in patients with left ventricular dysfunction and high left-heart resistive loads, as increasing the flow through the pulmonary circuit may worsen pulmonary vascular congestion by allowing for greater forward flow into an already weakened and overloaded LV [109]. Ongoing monitoring via POCUS and PAC can aid in tailoring therapy, avoiding complications, and allow for timely escalation to mechanical circulatory support (MCS) in refractory cases.
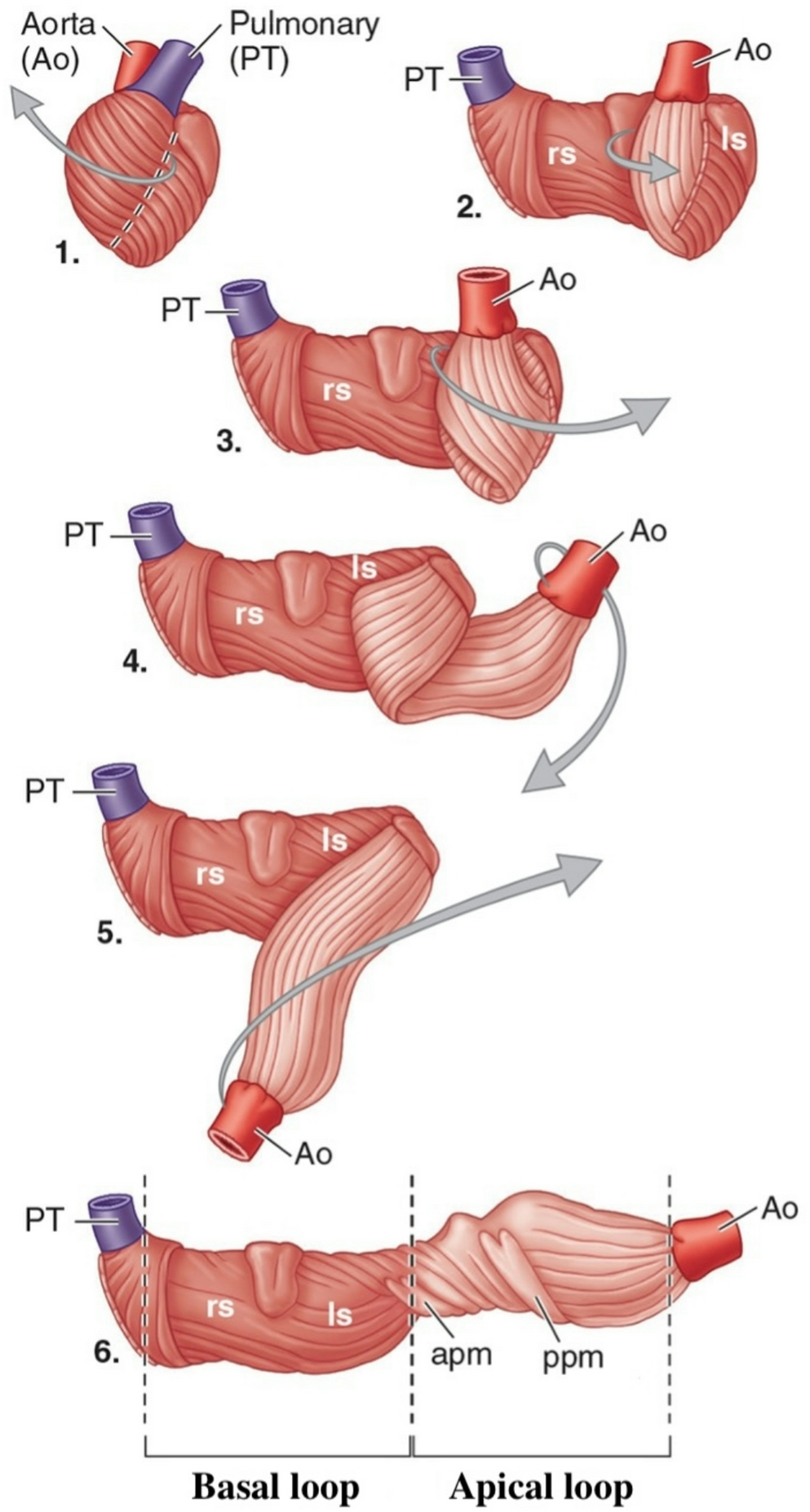
Enhancing RV ContractilityRV contractility is impaired in acute RVF due to RV free wall myocyte mechanical stretching, impaired oxygenation and cellular metabolic derangements. This can be improved through several targeted strategies, tailored to the underlying etiology, with improving LV contractility serving as a critical approach. As mentioned previously, studies suggest that the LV contributes up to 60% of the RVEF via IVS contraction, driven primarily by the helical fibers of the myocardium with significant contribution from the basal loop’s fiber architecture [2, 110]. Inotropic agents such as epinephrine, dobutamine and milrinone can improve RV function primarily by improving LV function through enhancing IVS contractility, rather than improving the function of an already distended RV free wall.
The choice of inotropic agent depends on several factors such as PVR, SVR and CO. Milrinone, a phosphodiesterase-3 inhibitor, is preferred in patients with high PVR and without systemic hypotension as it offers the highest reduction in PVR but causes peripheral vasodilation. Dobutamine, A β1-adrenergic agonist, improves contractility with minimal impact on PVR and minimal reduction of SVR. It is the ideal choice in patients with mild PVR elevations, normal to low SVR and low CO. In contrast, low-dose epinephrine is ideal for patients with low SVR, providing inotropic support without the systemic vasodilation associated with milrinone and dobutamine. However, higher doses of Epinephrine should be avoided in elevated-PVR states, as it worsens pulmonary vasoconstriction. Effective management balances IVS inotropic support with RV afterload reduction, while carefully monitoring for side effects like increased myocardial oxygen demand and tachyarrhythmias [106] (Table 1).
Table 1 Hemodynamic effects and the mechanism of action of commonly used inotropic agents used for the management of acute RVFCoronary PerfusionOptimizing coronary perfusion is critical to ensure adequate myocardial oxygen delivery and maintain CO in RVF. RV dilation and increased wall tension can impair coronary perfusion through mechanical compression exerted by the limited space of the pericardial sac. This effect is particularly pronounced in patients with coronary artery disease, where reduced myocardial oxygen supply may precipitate a critical decline in RV function. In cases of inferior myocardial infarction, timely revascularization can significantly improve outcomes.
Currently, there are no guidelines for the optimal BP targets in RVF, and the MAP target of 65 mmHg has been used universally in different types of shock to support perfusion [106, 111]. Unlike the left, right-sided coronary perfusion takes place during both systole and diastole, requiring optimization of MAP rather than SBP. The interplay between perfusion and congestion is demonstrated well by a retrospective study of pre-capillary PH patients with RVF admitted to an ICU, showing that patients with a dynamic MAP target, based on MAP = 60 + CVP to optimize systemic perfusion pressure (SPP), had lower in-hospital mortality and incidence of AKI compared with patients with static targets of MAP 65 or 70 [112]. Therefore, systemic hypotension should be avoided due to concern for hypoperfusion of the coronary circulation, kidneys, and bowels. When selecting inotropes and pressors, the goal is to optimize SPP by increasing SVR and RV contractility, with minimal increase in PVR, which may worsen RV failure by increasing RV afterload [106]. It is important to note that catecholamines increase myocardial oxygen demand, while vasoconstrictors may compromise microcirculation and tissue perfusion. Therefore, their use should be limited to the lowest effective dose and the shortest duration necessary [113].
Choice of VasopressorsIn the management of RVF with hypotension, initial treatment involves vasopressin, which reduces PVR while increasing SVR, thereby supporting SPP and coronary perfusion without exacerbating RV afterload. Low-dose epinephrine can be added to enhance these effects and provide inotropic support, improving CO while maintaining minimal impact on PVR. If hypotension persists, norepinephrine is titrated to achieve a MAP target for optimal SPP with minimal PVR increase, making it a first-line choice for persistent hypotension in RVF. Phenylephrine is not recommended, as it increases PVR, worsening RV afterload and potentially reducing CO. Similarly, methylene blue should be avoided due to its significant increase in PVR, which can further impair RV function. Dopamine and angiotensin II (ATII) are also contraindicated in RVF, as dopamine risks arrhythmias and variable PVR effects, while ATII increases both PVR and SVR, potentially straining the RV [88] (Table 2).
Table 2 Hemodynamic effects and the mechanism of action of commonly used vasopressor agents used for the management of acute RVFCorrection of Myocardial DepressionOf great importance is enhancing myocardial contractility by reversing conditions that directly result in reduction of myocardial contractility. Aggressive treatment of acidosis, hypoxia, and electrolyte imbalances such as hypokalemia and hypomagnesemia can often result in significant improvement in RV hemodynamics.
Rhythm control is another important factor in myocardial contractility. One of the characteristic anatomical changes in RVF is cardiac chamber dilation. Chamber wall stretch can lead to increased rates of both atrial and ventricular arrhythmias. These, in turn, can decrease myocardial contractility by disrupting coordinated contraction, increasing oxygen demand, and impairing coronary perfusion. In patients with RVF and atrial fibrillation (AF), RA emptying fraction is lower compared to patients without AF history [114]. Given the RV’s vulnerability, these effects are amplified, making effective arrhythmia management critical [106]. In the setting of hemodynamic compromise or arrest due to RVF, direct current cardioversion (DCCV) is the preferred initial treatment, as it rapidly restores sinus rhythm and optimizes coordinated ventricular contraction by improving cardiac output. This is in contrast to antiarrhythmic drugs, which may act more slowly and risk further hemodynamic instability. To maintain sinus rhythm post-DCCV, amiodarone is recommended as the first-line antiarrhythmic due to its minimal negative inotropic and chronotropic effects, preserving myocardial contractility and heart rate to support CO. In contrast, negative chronotropic and inotropic agents, such as beta-blockers and calcium channel blockers, are contraindicated because they reduce heart rate and contractility, further compromising cardiac output in an already impaired RV. Digoxin may be considered for rate control, as it offers mild positive inotropic effects that can support RV function; however, concerns about renal toxicity and increased mortality with chronic use limit its role to selected cases in which other rate-control agents are ineffective or contraindicated [115].
Mechanical Support in RVFThe introduction and evolution of MCS transformed care for refractory RVF. It reflects both technological advancement and deeper understanding of the complex structure–function interactions characterizing RVF physiology [116]. While cardiopulmonary bypass, extracorporeal membrane oxygenation (ECMO), ventricular assist devices (VAD) and intra-aortic balloon pumps (IABP) were available since the 1960’s [117], RV specific support devices were not available until the 1990’s. During this interim period, RVF was not yet recognized as a distinct clinical entity and most MCS efforts focused on LV or biventricular failure. The 1990’s saw the emergence of RV-specific MCS with the introduction of pulsatile right-ventricular assist devices (RVAD) [118]. Used as a bridge to transplant, these devices required complex surgery and large external pumps resulting in high rates of morbidity [119]. The TandemHeart was introduced in the late 1990’s and offered a percutaneous approach rather than surgical. Originally created for left atrial-to-femoral artery bypass, it was adapted to RVF by cannulating the right atrium to the pulmonary artery. The 2000’s saw a shift from pulsatile VADs to continuous flow devices, but this proved more useful for LV failure since the RV is more sensitive to changes in preload and afterload. The ImpellaRP was approved by the FDA in 2017, offering the ability to deliver adequate continuous flow to the PA from the RA percutaneously [2].
Effective Impella hemodynamic support is limited in high PVR conditions not responsive to pulmonary vasodilators and biventricular failure, limiting its use to RV infarction and post-thrombectomy [120, 121]. Additionally, its availability is limited due to its high cost and need for expertise. The ProtekDuo, introduced concurrently with the Impella RP, is generally preferred when prolonged support (> 7–10 days), concomitant oxygenation, early ambulation, or internal jugular access (e.g., in patients with IVC filters or severe obesity) is required [121, 122].
The last decade is characterized by the adoption of the idea of biventricular support with the development of the “Bi- PELLA” combining RV and LV Impellas allowing individual flow adjustment to each ventricle, with studies demonstrating improved survival. Recent advances in ECMO cannulation techniques, smaller more efficient circuits and its widespread availability, established ECMO as the MCS of choice in most cases of RVF. Despite ongoing research and innovation, the complex anatomy and physiology of the RV remain challenging for the development of a commercially viable long-term RVAD to date [2].
Respiratory Support StrategiesEndotracheal IntubationIn the event of hypoxemic respiratory failure in RVF patients, preoxygenation with HFNC is of paramount importance to improve oxygen reserve given the deleterious effects of hypoxia and PPV on RV function and hemodynamics as outlined in the previous sections. Endotracheal intubation of patients with acute RVF should be preferably undertaken by an intensivist who is experienced in both high-risk intubations and the hemodynamic implications of doing so in acute RVF. Some of the dangers of intubation in patients with acute RVF are the derivatives of supine positioning such as lung de-recruitment and upsurge in preload. Other risks stem from the use of induction agents such as propofol leading to decreased contractility and SVR, leading to coronary hypoperfusion resulting in further decrease in contractility which may eventually lead to hemodynamic collapse [123]. Even with successful intubation many dangers await in the minutes post intubation. The application of PPV causes an increase in intrathoracic pressure and increasing downstream pressure on hepatic veins and the IVC, leading to decreasing venous return and preload. These effects, coupled with the lingering effects of induction agents and the application of sedatives and analgesics post intubation, may lead to a delayed circulatory collapse many minutes post intubation. It is imperative to observe the patient closely in the post intubation period, add sedatives and analgesics in a stepwise fashion, and continue all RV off-loading therapies post-intubation. Steps must be taken to ensure proper intravenous access to prevent any interruptions in therapy and to facilitate the rapid application of vasopressor support if needed.
Ventilator ManagementPositive pressure ventilation is used in many critically ill patients and results in increased intrathoracic pressure leading to increased RV afterload [124]. The effects of PPV on RV hemodynamics are best explained by dividing the lung field into three vertical zones (Fig. 7), first conceptualized by West [17]. As hydrostatic pressure increases with gravity, the balance between ventilation and perfusion changes accordingly, whereby under normal conditions the alveolar pressure gradient is relatively similar to that of the arterial and the venous creating an ideal ventilation/perfusion (VQ) balance. In zone 1, where arterial and venous hydrostatic pressures are low compared to the alveolar pressure, the VQ is mismatched in favor of ventilation (this is also where pulmonary vascular capacity is capable of expanding in the event of increased volume to ameliorate the rise in PVR). On the other hand, in Zone 3, both arterial and venous pressures are higher than alveolar pressure, resulting in a VQ mismatch in favor of perfusion. With the introduction of PPV, the pressure relationships in the different lung zones change due to the increase in alveolar pressures. Zone 1 has further decrease in perfusion, tilting the VQ relationship further in favor of ventilation. In addition, Zone 1 becomes less available to accept more volume, resulting in the transmission of retrograde pressure into the RV, resulting in an increase in afterload. An additional effect of PPV is that Zone 2 becomes more like Zone 1 prior to the application of PPV, and Zone 3 becomes the area where VQ is most balanced. In situations of RVF with a large component of fluid overload, the presence of significant pulmonary effusions can be detrimental due to compression atelectasis, resulting in a decrease in functional pulmonary areas in zone 3, but also present as a target for rapid improvement by percutaneous drainage. It is important to note that the effects of PPV are seen in both invasive and non-invasive mechanical ventilation [125].
Fig. 7
West lung zones under normal conditions illustrating gravity-dependent pulmonary blood flow and ventilation-perfusion dynamics. Zone 1: Alveolar pressure exceeds pulmonary artery and venous pressures creating dead space of ventilated but poorly perfused area. Zone 2: pulmonary artery pressure exceeds alveolar pressure, but alveolar pressure greater than venous pressure, creating a balanced ventilation-perfusion zone. Zone 3: increasing gravity effect results in both arterial and venous pressures exceeding alveolar pressure, resulting in high perfusion relative to ventilation mismatch. When PPV is applied, particularly using high PEEP, alveolar distention may occur. This can lead to compression of extra-alveolar vessels and results in increased PVR, leading to redirection of blood flow into poorly ventilated lung regions and worsening V/Q, resulting in hypoxemia and hypercapnia. PA alveolar pressure, Pa pulmonary artery pressure, Pv pulmonary vein pressure. Adapted from [17]. Created in BioRender. Dodi, A. (2025) https://BioRender.com/ngngks2
Hypoxia and Acidemia Effects on PVRElevated RV afterload plays a pivotal role in the evolution of RVF, and its reduction is often very impactful. Hypoxia exerts significant influence on PVR, where alveolar hypoxia increases PVR to a greater degree compared with pulmonary arterial hypoxia. The pulmonary vasoconstrictive response to hypoxia is often accompanied and further potentiated by acidemia, hypercapnia, and atelectasis [106]. The pH of pulmonary capillary blood often changes in association with O2 content, which is particularly common during hypo- or hyperventilation and preexisting lung disease (source). Additional contributors of acidemia exacerbation in RVF result from retrograde hepatic venous congestion impairing citrate metabolism and lactate clearance. Another potential source of increased PVR is pulmonary endothelial injury resulting from multiple blood and platelet transfusions (source).
Comments (0)