
Remember me

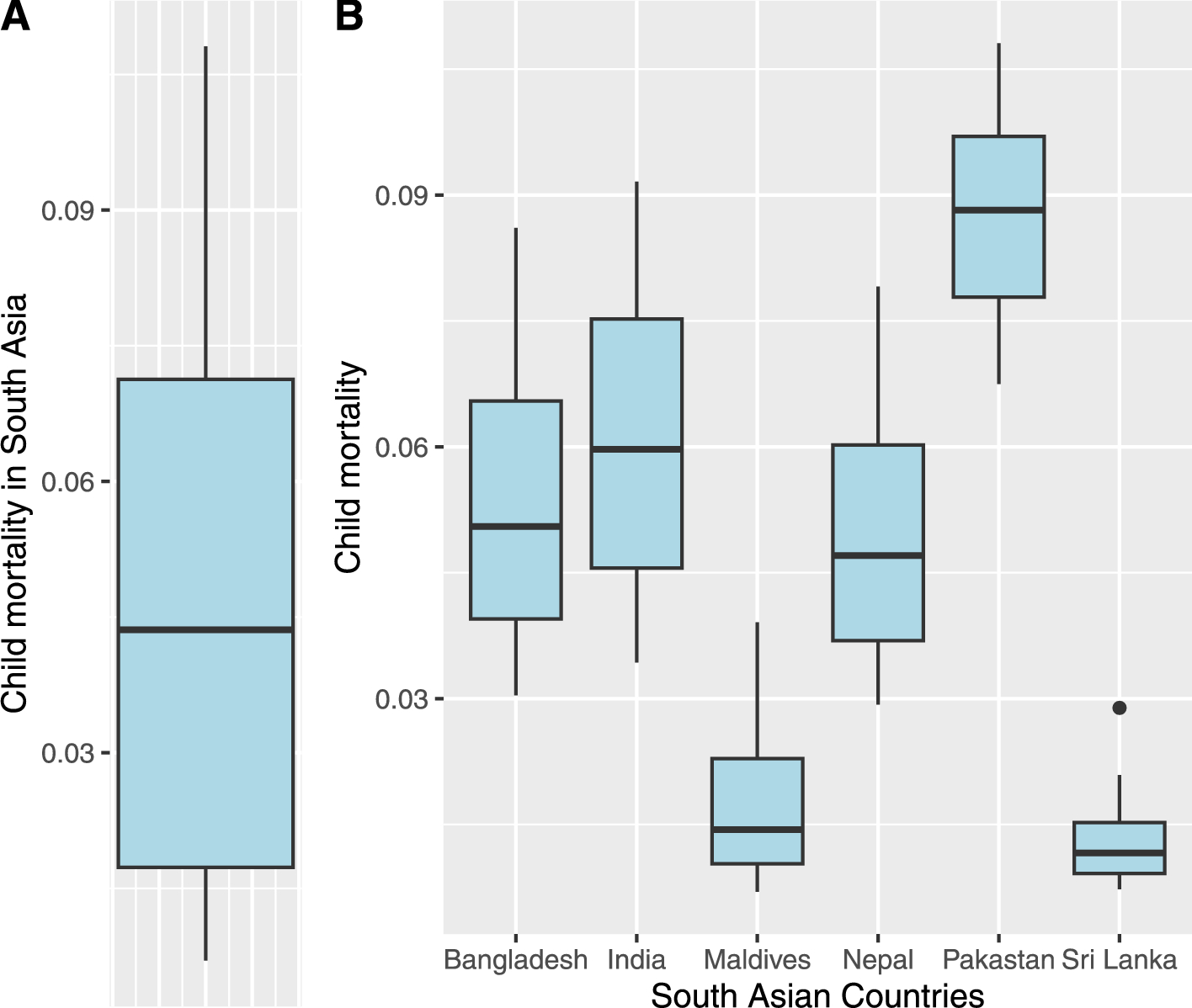
Child mortality rate data was taken from World Bank (The World Bank 2020). This data set was also used by Bam (2023b) in their study. The child mortality rate, expressed as deaths per 1000 births, is confined within the range of 0 and 1. The analysis covers the period from 2000, serving as the baseline, to 2020. This study focuses on six countries in the South Asian region: Pakistan, India, Sri Lanka, Bangladesh, the Maldives, and Nepal. The table presented in 4 reveals that the Maldives exhibits the highest health expenditures, while Bangladesh records the lowest. In terms of average years of schooling, Sri Lanka ranks highest, while Nepal has the lowest figures. Additionally, in terms of the HDI, Sri Lanka ranks highest, contrasting with Pakistan, which has the lowest HDI. For a detailed breakdown, please refer to Table 4. The box and whisker plot of overall child mortality rates in South Asia is presented in Fig. 1A, while the box and whisker plot of child mortality across South Asian countries is depicted in Fig. 1B. It indicates that the child’s overall mortality rate is slightly right-skewed. Pakistan experienced the highest rate compared to other countries, while the Maldives and Sri Lanka exhibit the lowest rates of child mortality. Following is the mixed effects model to analyze the association between the response variable child mortality rate (\(y_\)) and predictors time (\(x_\)), health expenditure (\(x_\)), average years of schooling (\(x_\)), and HDI (\(x_\)), controlling for subject-level clustering (countries);
$$\begin logit(\mu _)= \beta _0+\beta _1x_+\beta _2 x_+\beta _3 x_+\beta _4 x_+u_i, \end$$
(16)
where \(\mu _,\) is the conditional mean of the response variable child mortality, i = 1, ..., 7, j = 0,...,19. Here 0 represents the base year 2000. \( u_i \) is a random intercept that follows a normal distribution with mean 0 and standard deviation \( \sigma _u^2 \).
Table 4 Summary statistics of predictorsFig. 1
Box and whisker plot of child mortality rates in South Asia (A) and across South Asian Countries (B)
The results of both models were presented in Table 5. It encompasses all parameter estimations, including 95% credible intervals, standard errors, effective sample size, Gulbin and Rubin diagnostics as well as metrics such as WAIC and LOOIC. All diagnostics were satisfactory; for example, the effective sample size exceeded 10% of the total samples. Trace plots and ACF plots demonstrated satisfactory MCMC convergence, as depicted in Figs. 2, 3, and 4, 5, respectively.
Based on LOOIC and WAIC, NULMM outperforms ULMM (see Table 5). Results further show that on average, the child mortality rate linearly declines over time. Furthermore, there is a negative relationship between the conditional mean of child mortality and predictors: health expenditure, average years of schooling, and human development index.
Table 5 Posterior summary statistics of child mortality analysisFig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5 6.2 Analysis of COVID-19 mortality across South Asian countries
6.2 Analysis of COVID-19 mortality across South Asian countriesData for this study was taken from Our World in Data (Mathieu et al. 2020). The proposed response variable is COVID-19 mortality rate per 100,000, and time, scaled GDP per capita, hospital bed count per 1000, and the proportion of people aged 65 and older are proposed predictors. Scaled GDP is obtained by dividing GDP per capita by 1000, effectively representing GDP in thousands of dollars. Hospital bed count is measured as the number of available beds per 1000 population. Age is measured as the proportion of the population aged 65 years and older. Since the NULMM requires a response variable must be bounded within the interval of 0 and 1 (\(0<y_\le 1\)). There are some 0 s in the COVID-19 mortality rates, thus it needs adjustment. To adjust it, we employed the corrections factor suggested by Verkuilen and Smithson (2012). According to their recommendations, it should be adjusted using the following relationship
$$\begin Y_} = \frac}(N-1) + 0.5}, \end$$
where \(Y_}\) is the new corrected response variable, \(Y_}\) is the old response variable, and \(N\) is the sample size.
Following is the NULMM used to analyze the association between the response variable COVID-19 mortality rate (\(y_\)) and predictors: time (\(x_\)), GDP (\(x_\)), hospital bed count (\(x_\)), and age (\(x_\)), controlling for subject-level clustering (countries)
$$\begin logit(\mu _)= \beta _0+\beta _1x_+\beta _2 x_+\beta _3 x_+\beta _4 x_+u_i \end$$
(17)
where, \(\mu_\), is the conditional mean of the response variable child mortality, i= 1,2....7, j=0,1....24. Here 0 represents the base month (January 2020). \( u_i \) is a random intercept that follows a normal distribution with mean 0 and standard deviation \( \sigma _u^2 \).
Before analyzing the association, we explored the death rate variable (deaths per 100,000), as presented in Fig. 6. The pattern of death rates is relatively uniform across all countries in the South Asian region, with Afghanistan experiencing the highest deaths compared to other countries, while Sri Lanka experienced the least. Similarly, the average GDP across South Asian countries stands at US$ 5659 with a standard deviation of 3308.02. Among these countries, Maldives boasts the highest GDP at US$ 11,669, while Afghanistan has the lowest GDP at US$ 1804. Maldives was excluded because of the unavailability of data. Regarding hospital bed capacity, on average, there are 1.147 hospital beds per 1000 people with a standard deviation of 1.089. Nevertheless, Sri Lanka stands out with the highest number of hospital beds, at 3.6 beds per 1000 people, while Nepal has the fewest beds, with only 0.3 beds per 1000 people. The South Asian region exhibits an average of 5.561% of its population aged 65 and older, with a standard deviation of 2.119%. Notably, Sri Lanka has the highest proportion, with 10.07% of its populace falling into this age group, whereas Afghanistan has the lowest with 2.581%.
The results of NULMM and ULMM were presented in Table 6. All diagnostic measures indicated satisfactory convergence of the MCMC. For instance, the effective sample size exceeded 10% of the total samples. Trace plots and ACF plots illustrated satisfactory MCMC convergence, as shown in Figs. 7, 8, 9, and 10, respectively.
While comparing both models, LOOIC and WAIC of NLUMM were less than ULMM (refer to Table 6). According to the posterior summary statistics, the mortality rate of COVID-19 has been observed to escalate over the initial two-year period. Additionally, GDP and the number of hospital beds appear to act as protective factors against COVID-19 mortality, as they exhibit a negative correlation with mortality rates. Conversely, the proportion of elderly individuals within a country is identified as a risk factor for COVID-19 mortality.
Fig. 6
Spaghetti plot of COVID-19 mortality rate
Fig. 7 Fig. 8
Fig. 8 Fig. 9
Fig. 9 Fig. 10
Fig. 10 Table 6 Posterior summary statistics of COVID-19 mortality
Table 6 Posterior summary statistics of COVID-19 mortality
Comments (0)