Olmesartan-associated enteropathy presenting with metabolic acidosis and acute kidney injury requiring hemodialysis: a rechallenge-confirmed case
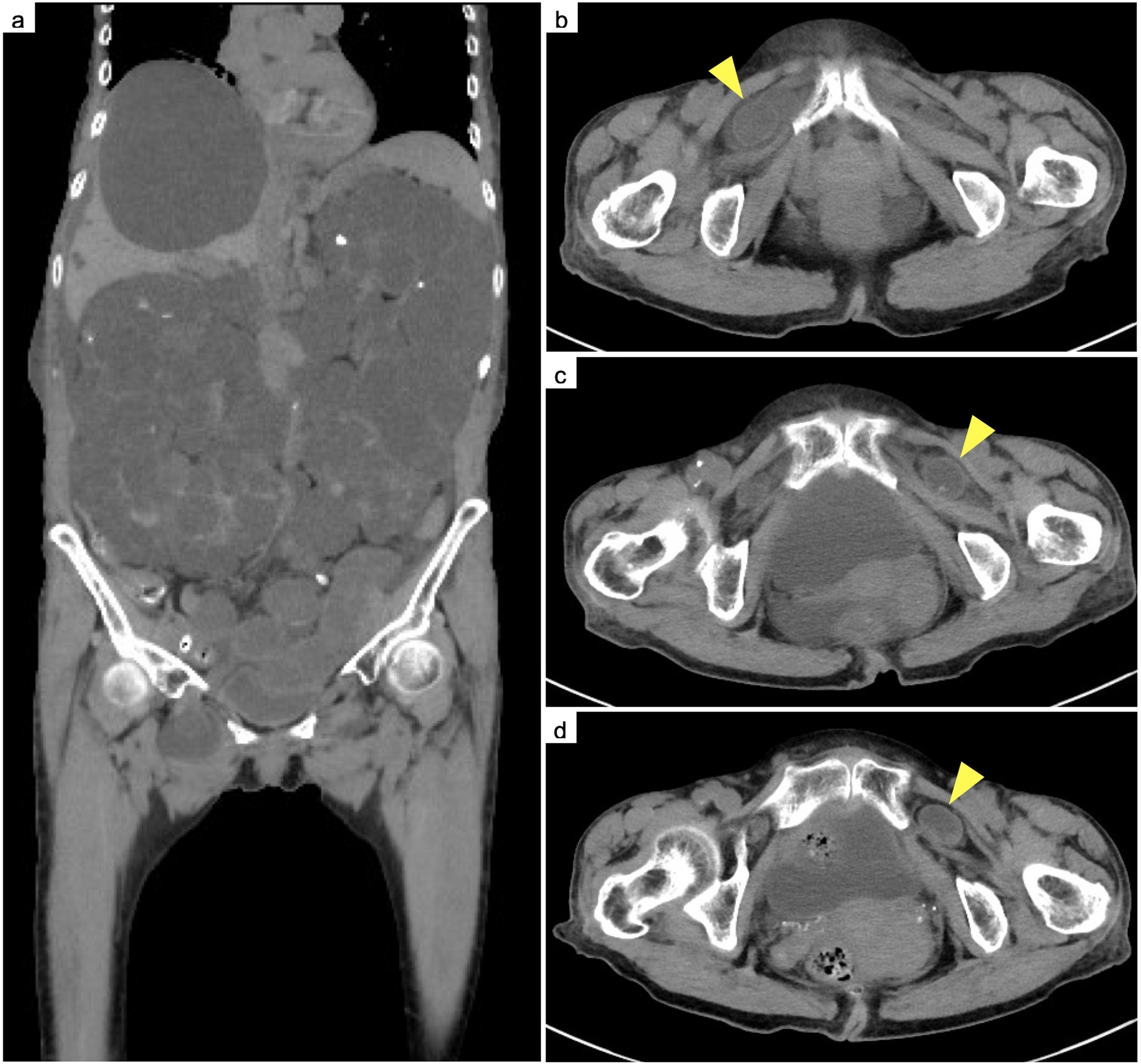
Olmesartan-associated enteropathy (OAE) is a delayed-onset drug-induced intestinal disorder that mimics celiac disease and may cause severe diarrhea, electrolyte imbalance, and prerenal acute kidney injury (AKI). Although rare, recognition is essential because timely drug withdrawal is curative. An 82-year-old man on long-term olmesartan therapy developed one month of watery diarrhea, weight loss, and hypotension, leading to hyperchloremic metabolic acidosis and severe AKI (serum creatinine (Cr) 6.77 mg/dL). Symptoms resolved after discontinuation of olmesartan. After discharge, olmesartan was restarted, resulting within days in recurrent diarrhea, profound mixed metabolic acidosis (pH 7.01; HCO₃⁻ 4.7 mmol/L; anion gap 23.3 mEq/L), and severe AKI (Cr 12.25 mg/dL), requiring emergency hemodialysis. During the second hospitalization, temporary re-initiation of olmesartan again precipitated rapid clinical deterioration, and the need for another hemodialysis session. Computed tomography demonstrated duodenal–ileal wall thickening, while colonoscopy and biopsies remained normal. Permanent discontinuation of olmesartan led to complete resolution without recurrence for over one year. This case highlights a severe form of OAE presenting with recurrent life-threatening metabolic acidosis and AKI requiring hemodialysis, with a dechallenge–rechallenge relationship that strongly suggested a causal association with olmesartan. In older adults with chronic diarrhea, weight loss, electrolyte disturbances, or unexplained AKI, angiotensin II receptor blocker-induced enteropathy should be considered, and immediate drug withdrawal is critical to prevent renal deterioration.





Comments (0)