
Remember me




Autosomal dominant tubulointerstitial kidney disease due to UMOD variants (ADTKD-UMOD) is a hereditary nephropathy caused by pathogenic variants in the UMOD gene, which encodes the glycoprotein uromodulin and is located on chromosome 16p12. Clinically, it is characterized by chronic kidney disease (CKD) and hyperuricemia [1]. CKD in ADTKD-UMOD typically progresses during adulthood, with a reported median age at diagnosis of 30.5 years [2] and a median age at onset of kidney failure of 47 years [3].While there have been reports of ADTKD identified during childhood through family screening at early stages of CKD, progression to kidney failure during childhood is rare [1]. Here, we report a sporadic pediatric case of ADTKD-UMOD diagnosed during the evaluation of advanced CKD.
Case Presentation.
A 7-year-old girl, born to healthy, non-consanguineous Japanese parents, was brought to the emergency department for afebrile seizure. The seizure resolved spontaneously, and brain MRI and EEG revealed no abnormalities. Subsequently, the seizures were diagnosed as Panayiotopoulos syndrome. As an incidental finding, her serum creatinine level was elevated at 1.57 mg/dL (creatinine-based eGFR: 28 mL/min/1.73 m²), consistent with CKD stage 4. She was referred to our hospital for further evaluation.
She had no history of abnormal urinalysis findings, and no family history of kidney disease or dialysis. Her height was 115 cm (–0.6 SD) and weight was 18.5 kg (–1.0 SD). No abnormalities were found on physical examination. Laboratory tests showed a creatinine-based eGFR of 26 mL/min/1.73 m², cystatin C-based eGFR of 31 mL/min/1.73 m², hemoglobin 9.3 g/dL, and uric acid 9.3 mg/dL. Early morning urine showed a specific gravity of 1.006, indicating hyposthenuria.
Ultrasonography indicated that the left kidney measured 6.3 × 3.9 cm (–2.3 SD) and the right kidney measured 6.9 × 3.9 cm (–1.6 SD), suggesting that the kidneys were small to normal in size. Increased echogenicity and the presence of several small cysts were also observed. These findings were suggestive of nephronophthisis. In addition, punctate echogenic foci consistent with calcifications were observed within the parenchyma. No abnormalities were found in the bladder, ureters, liver, or other organs. Otolaryngologic and ophthalmologic evaluations revealed no extrarenal manifestations.
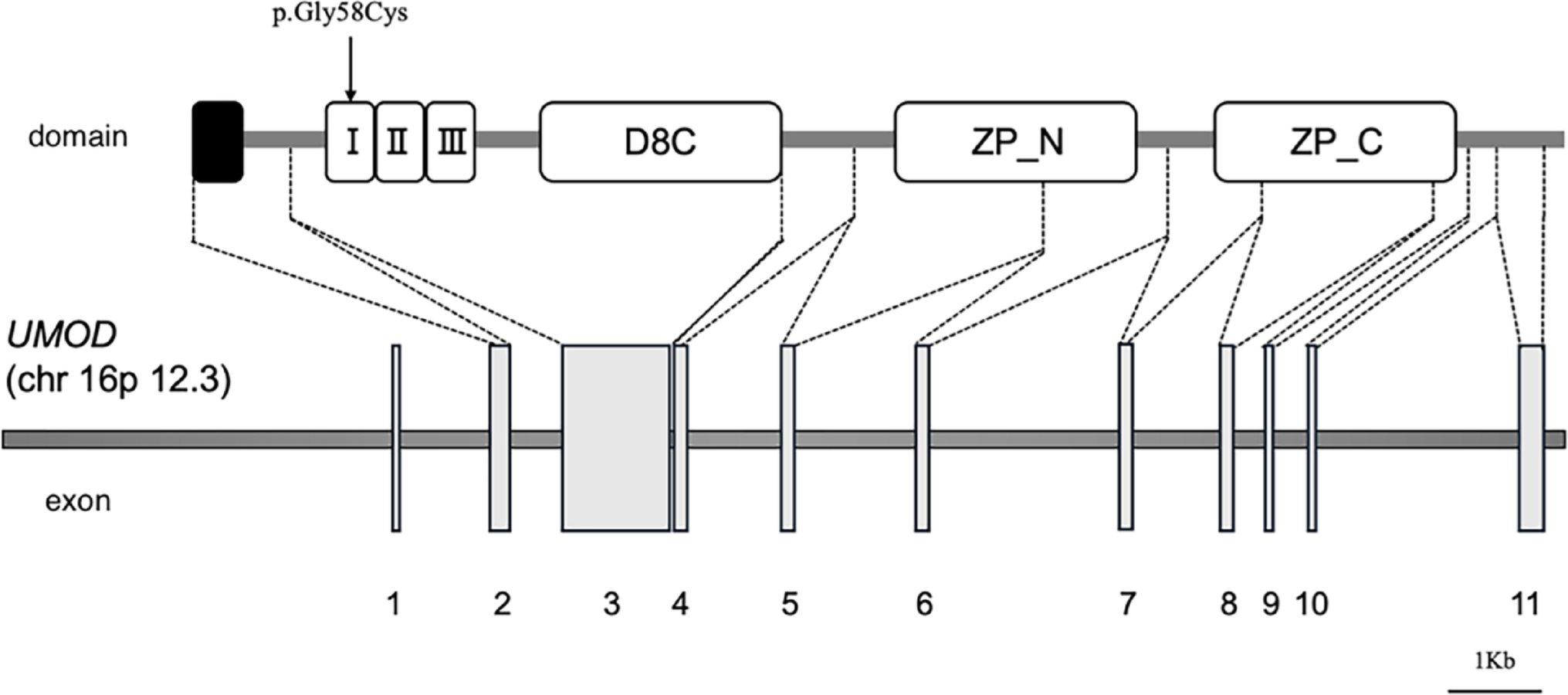
Due to the sporadic nature of the case and the presence of normal to small-sized kidneys with cysts and progressive CKD in childhood, nephronophthisis was initially suspected. However, genetic testing for nephronophthisis-related genes, conducted with parental consent, revealed no pathogenic variants. Subsequently, targeted panel exome analysis covering 187 genes related to congenital anomalies of the kidney and urinary tract (CAKUT) and cystic kidney diseases was performed in the proband. Sanger sequencing was then conducted for the patient and both parents, and the variant was detected only in the patient but not in the parents. This confirmed that it was a de novo variant, c.172G > T, p.Gly58Cys, in the EGF-like domain 1 of the UMOD gene (Fig. 1) [4]. Neither parent carried this variant. Based on the results of genetic analysis, the patient was diagnosed with ADTKD-UMOD. Treatment for CKD was initiated with oral sodium bicarbonate and febuxostat. Subsequent monitoring of renal function revealed a decline in eGFR to 19 mL/min/1.73 m² 1 year and 2 months after the initial visit to our hospital, at which point the patient was registered for deceased donor kidney transplantation.
Fig. 1
Schematic representation of the UMOD gene structure and corresponding protein domains
The UMOD protein, which consists of three epidermal growth factor (EGF)–like domains, a D8C domain, and a zona pellucida (ZP) domain. The variant identified in this case, p.Gly58Cys (arrow), is located within EGF-like domain 1, which is encoded by exon 3
I, EGF-like domain 1; II, EGF-like domain 2; III, EGF-like domain 3; D8C, central domain; ZP_N, N-terminal subdomain of the zona pellucida domain; ZP_C, C-terminal subdomain of the zona pellucida domain
Comments (0)